 |
Case Report
Adult intussusception due to an inflammatory fibroid polyp, an uncommon cause of acute bowel obstruction
1 Department of General Surgery, Hospital Vozandes Quito, Quito, Ecuador
2 PGY4 Resident General Surgery, P.U.C.E, Quito, Ecuador
3 Universidad Internacional del Ecuador, Quito, Ecuador
Address correspondence to:
Gabriel A Molina
PGY4 Resident General Surgery, P.U.C.E, Quito,
Ecuador
Message to Corresponding Author
Article ID: 100038S05MA2019
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Araujo MO, González HR, Ayala AV, Vayas R, Rodriguez EX, Molina GA. Adult intussusception due to an inflammatory fibroid polyp, an uncommon cause of acute bowel obstruction. Edorium J Surg 2019;6:100038S05MA2019ABSTRACT
Introduction: Intussusception is a common phenomenon in children but rare in adults, however when it happens, it usually presents with symptoms clinically indistinguishable from an acute bowel obstruction making preoperative diagnosis challenging. In rare occasions, an inflammatory fibroid polyp can be a lead point for intussusception. Most small bowel inflammatory fibroid polyps are asymptomatic and usually go undetected until they produce symptoms based on their size and location. Surgery is the definitive treatment of adult intussusceptions. Complete bowel resection with oncological principles is necessary as malignancy must always be suspected.
Case Report: We present the case of a 37-year-old female, who presented to the emergency room with acute bowel obstruction. An entero-enteric intussusception was discovered due to an inflammatory fibroid polyp. After successful surgery, she underwent complete recovery.
Conclusion: A high clinical awareness along with complete knowledge of the abdominal pathology is required for all surgeons when approaching a patient with symptoms of bowel obstruction. Even though inflammatory fibroid polyps are a rare pathology, they can cause potentially lethal scenarios and must always be considered in the differential diagnosis of bowel obstruction.
Keywords: Adult intussusception, Bowel obstruction, Inflammatory fibroid polyps
INTRODUCTION
Inflammatory fibroid polyps are rare benign tumors of the gastrointestinal tract, they regularly appear in the stomach however any part of the bowel can be involved, they are usually asymptomatic however due to their wide clinical spectrum they can mimic various abdominal pathologies including intussusception [1],[4], as intussusception is uncommon in adults, diagnosis and treatment are often delayed [2],[3]. We present the case of a 37-year-old female with an entero-enteric intussusception caused by an inflammatory fibroid polyp, after successful surgery patient underwent full recovery.
CASE REPORT
Patient is a 37-year-old female without any past medical history, she presented to the emergency room with a four-day history of mild lower abdominal pain, constipation, and inability to pass gas. Twenty-four hours prior to her admission, the pain became worse and severe episodes of bilious vomits appeared. On clinical examination a dehydrated and tachycardic patient was encountered, her abdomen was distended and diffusely tender also and no bowel sounds were detected. Inguinal region examination did not reveal any hernias and on digital rectal examination, her rectum was empty.
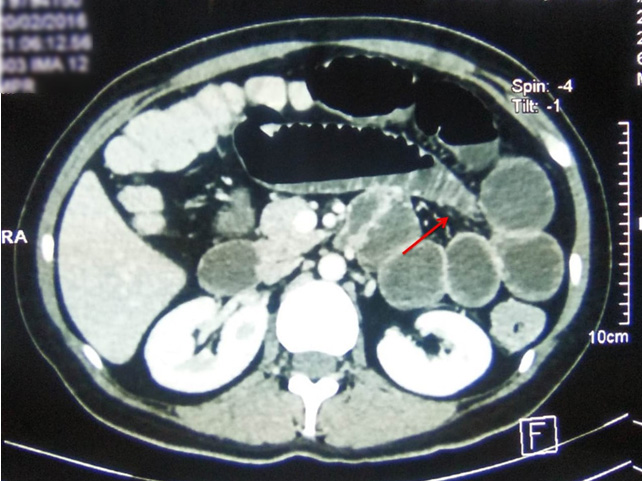
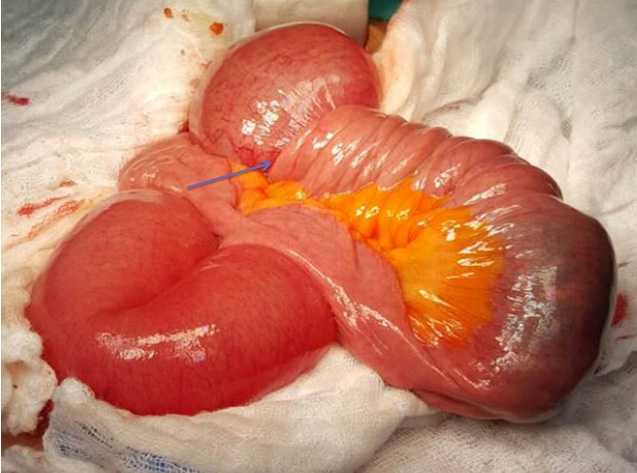
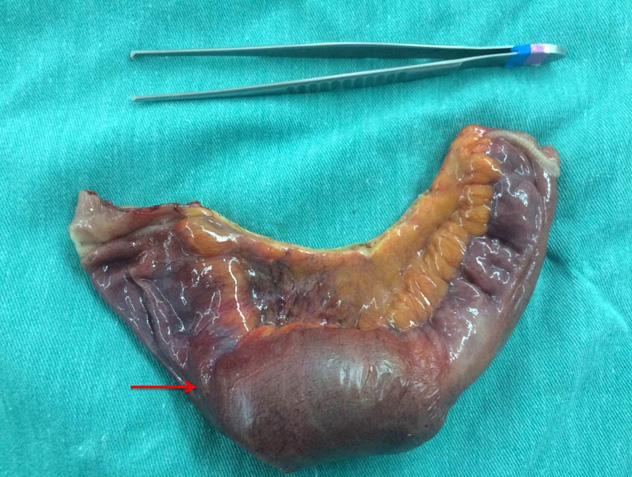
Complementary exams showed leukocytosis with neutrophilia, an abdominal X-ray revealed multiple dilated loops of small bowel in her right lower quadrant, and a contrast-enhanced abdominal computed tomography (CT) unveiled complete bowel obstruction, a transition point was discovered in the small bowel. There was an abrupt change in caliber between the proximal dilated bowel loops and collapsed distal bowel (Figure 1). After adequate reanimation, surgery was decided. At laparotomy, most of the loops of small bowel were dilated and an entero-enteric intussusception was discovered 60 cm proximal to the ileocecal valve (Figure 2). The compromised bowel was necrotic however no perforation was discovered, also a 6×4 cm soft intraluminal mass was discovered within the intussusception. No other masses of lymph nodes were discovered. From there surgery was straightforward, complete resection of the compromised bowel with a 5 cm margin was performed and a side to side primary anastomosis with a 50 mm linear autosuture (Ethicon Inc., Somerville, NJ, USA) was completed (Figure 3). Pathology exposed a 6×5×2 cm mucosal polypoid lesion, it contained edematous stroma with spindleshaped stromal cells and lymphoid nodules. On immunohistochemical analysis, the cells showed positivity for CD34 and were negative for CD117, S100, and smooth muscle actin. Inflammatory fibroid polyp causing small bowel intussusception was the final diagnosis. Her postoperative course was uneventful, sips of liquids were initiated on the second postoperative day and after full diet was tolerated she was discharged. On follow-up controls the patient is doing well.
DISCUSSION
Intussusception was first described by Barbette et al. in 1674, as an invagination of a segment of bowel into the lumen of an adjacent portion [1],[2]. This condition mostly affects pediatric patients, nonetheless, adults can be affected in less than 5% of all cases of intussusception [2]. Unlike what happens in children where 90% of childhood intussusception are idiopathic, in adults the majority (63%) of adult intussusception is tumor-related and up to 50% of them are malignant [1],[3]. Although the exact mechanism leading to intussusception is not known, it is believed that any condition in the bowel wall or within its lumen that changes the normal pattern of peristalsis is able to initiate an invagination process, once the invagination process has started the normal physiologic peristalsis promotes extension of the invagination to involve greater segments of the intestine, mesentery, and blood vessels [2].
First described by Vanek et al. in 1949 as a rare mesenchymal lesion in the gastrointestinal tract, inflammatory fibroid polyps (IFPs) are lesions that are thought to appear due to trauma, allergic reaction, genetic tendency, bacterial, physical, or chemical stimuli [4],[5]. Although they may occur in any part of the gastrointestinal tract, they are most commonly located in the stomach [6]. Gastric and colon IFPs are usually recognized incidentally, whereas small intestinal lesions are often encountered in the setting of intussusception [4],[6]. As it was found in our patient. They are submucosal lesions formed by multiples spindle cells and a prominent vasculature, they show immunoreactivity for CD34 and absence of CD117 and S-100 protein [4]. As it was discovered our case. IFPs are usually asymptomatic, however, their clinical spectrum depends on the location and size of the tumor, IFPs do not recur after surgical resection [7].
When intussusception happens on an adult patient they present as an emergency with a clinical picture of intestinal obstruction, adult intussusception causes less than 1% of all bowel obstructions [1]. It usually affects patients between 40 and 50 years, with a slight male predominance [2]. The most common symptoms include abdominal pain, nausea, vomiting, abdominal fullness, and tenderness. Preoperative diagnosis of intussusception in adults is difficult as it is a rare disease with nonspecific clinical signs and symptoms [1],[8]. Complementary exams including X-rays, ultrasonography, small bowel series, barium enema, and colonoscopy can aid in the diagnosis, but abdominal CT is currently considered as the most sensitive radiologic method to confirm intussusception, with a reported diagnostic accuracy of 58–100% [3]. In our patient, CT revealed bowel obstruction, however, intussusception was not recognized in the preoperative period. Surgery remains the definite treatment when approaching adult intussusception, reduction, followed by resection should be performed since the main causes are due to malignant tumors [2].
In our patient, acute abdominal obstruction was suspected, and after surgery intussusception was discovered, bowel resection was achieved and the patient completely recovered.
CONCLUSION
A high clinical awareness along with complete knowledge of the abdominal pathology is required when treating patients with symptoms of bowel obstruction, as many pathologists can mimic this condition. Also, even though inflammatory fibroid polyps are a rare pathology, they can cause potentially lethal scenarios. Adult intussusception must always be considered in the differential diagnosis of bowel obstruction.
REFERENCES
1.
Hong KD, Kim J, Ji W, Wexner SD. Adult intussusception: A systematic review and meta-analysis. Tech Coloproctol 2019:23(4):315–24. [CrossRef]
[Pubmed]

2.
Honjo H, Mike M, Kusanagi H, Kano N. Adult intussusception: A retrospective review. World J Surg 2015;39(1):134–8. [CrossRef]
[Pubmed]
3.
Lianos G, Xeropotamos N, Bali C, Baltoggiannis G, Ignatiadou E. Adult bowel intussusception: Presentation, location, etiology, diagnosis and treatment. G Chir 2013;34(9–10):280–3.
[Pubmed]
4.
Liu TC, Lin MT, Montgomery EA, Singhi AD. Inflammatory fibroid polyps of the gastrointestinal tract: Spectrum of clinical, morphologic, and immunohistochemistry features. Am J Surg Pathol 2013;37(4):586–92. [CrossRef]
[Pubmed]
5.
Carvalho A, Leitão P, Pinheiro J, et al. Small bowel intussusception in 2 adults caused by inflammatory polyps. Radiol Case Rep 2017;12(4):710–4. [CrossRef]
[Pubmed]
6.
Akbulut S. Intussusception due to inflammatory fibroid polyp: A case report and comprehensive literature review. World J Gastroenterol 2012;18(40):5745–52. [CrossRef]
[Pubmed]
7.
Han GJ, Kim JH, Lee SS, Park SH, Lee JS, Ha HK. Inflammatory fibroid polyps of the gastrointestinal tract: A 14-year CT study at a single institution. Abdom Imaging 2015;40(7):2159–66. [CrossRef]
[Pubmed]
8.
Kang SH, Kim SW, Moon HS, et al. Inflammatory fibroid polyp in the jejunum causing small bowel intussusception. Ann Coloproctol 2015;31(3):106–9. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Milton O Araujo - Substantial contributions to conception and design, Drafting the article, Final approval of the version to be published
Hernán R González - Substantial contributions to conception and design, Interpretation of data, Drafting the article, Final approval of the version to be published
Andrés V Ayala - Substantial contributions to conception and design, Revising it critically for important intellectual content, Final approval of the version to be published
Rafaela Vayas - Substantial contributions to conception and design, Final approval of the version to be published
Esteban X Rodriguez - Drafting the article, Final approval of the version to be published
Gabriel A Molina - Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Source of SupportNone
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 Milton O Araujo et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



