 |
Case Report
Autoimmune pancreatitis: A challenging diagnosis
1 MD, Department of General Surgery, Hospital Metropolitano, Quito, Ecuador
2 Department of Internal Medicine, Division of Radiology, Quito, Ecuador
3 MD, Department of General Surgery, Attending Surgeon, PUCE, Quito, Ecuador
4 MD, Attending, Surgeon, Iess Quito Sur and Digeslap Center, Quito, Ecuador
Address correspondence to:
Gabriel A Molina
MD, Attending Surgeon, Iess Quito Sur and Digeslap Center, Quito,
Ecuador
Message to Corresponding Author
Article ID: 100041S05FS2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Serpa FI, Armijos CA, Cueva ML, Burbano CE, Molina GA. Autoimmune pancreatitis: A challenging diagnosis. Edorium J Surg 2020;7:100041S05FS2020.ABSTRACT
Autoimmune pancreatitis (AIP) is a rare form of chronic pancreatitis. However, due to its wide spectrum of clinical and radiological characteristics, it can mimic pancreatic malignancies that could expose patients to unnecessary therapies if it is misdiagnosed. Unlike pancreatic malignancies, AIP adequately responds to steroid therapies. Diagnosis is challenging as pathological samples are usually needed to confirm the diagnosis. A high index of suspicion is needed as the diagnosis of AIP can easily be missed. We present the case of a 54-year-old patient, who presented with weight loss, abdominal pain, and asymptomatic jaundice. A pancreatic malignancy was suspected after an abdominal computed tomography (CT). Nonetheless, after a careful examination, AIP was detected and treated.
Keywords: Autoimmune pancreatitis, IgG4, Pancreas, Pancreatitis, Steroids
INTRODUCTION
Autoimmune pancreatitis is a rare kind of chronic pancreatitis which responds adequately to steroid therapy. This disease can be part of a multiorgan disorder that can manifest beyond the pancreas, called IgG4-related disease [1],[2]. Autoimmune pancreatitis can mimic pancreatic cancer, and its accurate diagnosis is important to avoid accidental surgery [1]. We present the case of a 54-year-old patient, for whom a pancreatic malignancy was suspected due to asymptomatic jaundice, weight loss, and a heterogeneous pancreas observed in a CT. Autoimmune pancreatitis was finally diagnosed and treated accordingly.
CASE REPORT
The patient is a 54-year-old male without any past medical history. He had a 6-month history of anorexia, severe weight loss (22% of previous weight) and intermittent episodes of mild abdominal pain. One week before presenting to the emergency room he noted a yellowing of his eyes and skin. On clinical examination, a malnourished patient with jaundice was encountered. The abdominal examination was unremarkable, and no lymph nodes or masses were identified. Laboratory exams revealed a cholestatic pattern with elevated conjugated bilirubin (21 mg/dL), gamma-glutamyl transferase (1359 U/L) and alkaline phosphatase (567 IU/L). Lipase and amylase were normal (56 and 102 U/L), yet Ca 19-9 and carcinoembryonic antigen (CEA) were mildly elevated (70 U/L and 25 ng/mL).
Due to this, an abdominal echography was performed and unveiled a normal gallbladder with a 13 mm common bile duct. An abdominal contrast-enhanced CT was requested, and it exposed a dilated common bile duct with a heterogeneous pancreas which was enlarged and surrounded by inflammatory tissue. However, no masses or lymph nodes were identified. A magnetic resonance cholangiopancreatography (MRCP) was requested, revealing a narrowing of the bile duct near its distal end with a 0.25 mm pancreatic duct. Based on these findings, an endoscopic retrograde cholangiopancreatography was performed and confirmed the bile duct stricture in its distal end. A plastic stent was placed and several biopsies were taken from the head of the pancreas with the aid of endoscopic ultrasound.
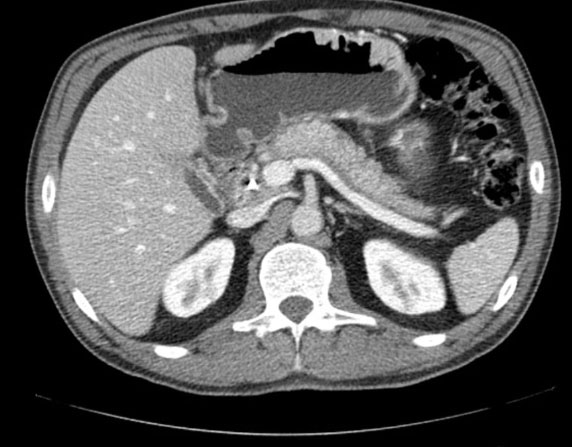
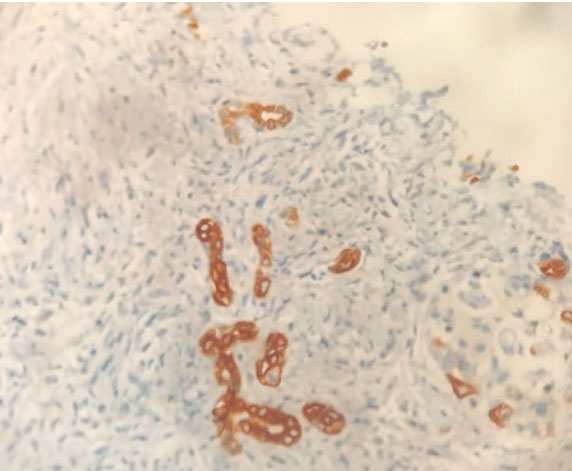
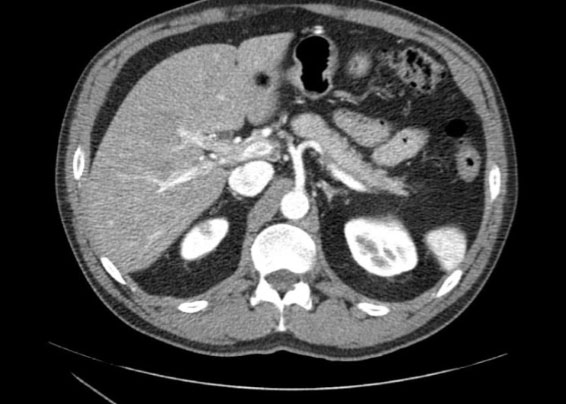
Overall, the complementary images were insufficient to establish a definitive diagnostic. Due to the unavailability of immunohistochemistry assays or a pathologist’s opinion on location, as the patient presented with severe weight loss and painless obstructive jaundice, he was misdiagnosed with a suspected pancreatic malignancy and surgical plans were discussed with the patient and his family. Because the patient was undecided about surgery, he sought a second opinion and came to our department. He provided us with the pathology samples and a new CT was performed (Figure 1). The pancreas appeared heterogeneous, surrounded by an inflammatory halo, yet no masses were found. Pathology reported pancreatic cells surrounded by severe inflammatory tissue. The pancreatic glands were enlarged, and yet the surrounding tissue was fibrotic and cells showed positivity for IgG4 (Figure 2). A type 1 autoimmune pancreatitis was suspected as serum IgG4 levels were high (over 400 mg/dL) and no evidence of malignancy was discovered on complementary exams. The patient underwent a 2-week steroids therapy (40 mg/day) which produced an observable clinical and radiological improvement (Figure 3). On follow-up controls and six months after initial diagnosis, the patient is performing well on steroid therapy (2.5 mg/day), jaundice has ceased (Total bilirubin 0.8 mg/dL), liver enzymes are normal and he has regained his previous weight.
DISCUSSION
Pancreatic cancer is the fourth leading cause of cancer-related deaths in western countries, with an overall 5-year survival rate of approximately less than 10%. The reasons for this poor survival rate are multifactorial including nonspecific symptoms, late diagnosis, and the close proximity of major blood vessels which can be invaded by this tumor. To this date, surgical resection is the only potential cure for pancreatic cancer, making early diagnosis a priority [1]. The term AIP was first proposed in 1995 by Yoshida et al. when they described a fibroinflammatory disease of the pancreas of possible autoimmune origin. Following investigations demonstrated that AIP is part of a multiorgan disorder called IgG4-related diseases [1],[2]. Autoimmune pancreatitis has been classified into two different kinds based on clinical, serological, radiological, and pathological characteristics. In type 1 AIP, the pancreas is affected as part of a systemic IgG4-positive disease, also known as lymphoplasmacytic sclerosing pancreatitis. On the other hand, type 2 AIP is characterized by idiopathic duct-centric pancreatitis [3]. Patients with type 1 AIP usually present with a history of obstructive jaundice, abdominal pain, and acute pancreatitis; however, due to its wide spectrum of symptoms, it can also mimic a malignant disease [1],[4], as was thought for our patient. Since diagnosis is based on pathological findings, multiple guidelines have been developed to aid clinical diagnosis. These include invasive and noninvasive methods, such as imaging, serology, steroid therapy trialing, and biopsy [2],[5].
Pancreatic imaging irregularities are found in up to 85% of patients with AIP. Computed tomography and MRCP can reveal diffuse parenchymal enlargement with delayed enhancement [6]. Enlargement is usually accompanied by the effacement of the lobular contour of the pancreas, giving the gland a “featureless” or “sausage-shaped” appearance [2]. On certain occasions, a halo can be observed which is strongly suggestive of AIP. Endoscopic retrograde cholangiopancreatography (ERCP) and endoscopic ultrasound can also aid the diagnosis [2],[3]. Imaging is also critical in the evaluation of patients with suspected pancreatic cancer, however, unlike in AIP, CT usually shows a hypoattenuating pancreatic mass associated with pancreatic duct dilatation, atrophy of the upstream pancreas, yet the detection of pancreatic malignancies ranges from 76% to 96% for CT and from 83% to 93.5% for magnetic resonance imaging (MRI) [7],[8].
IgG4 typically accounts for less than 5% of all the total serum IgG in normal patients. Increases in IgG4 can be encountered in patients with AIP, yet IgG4 titers are not specific to AIP and can also be seen in patients with cancer, which is why serology data should be used together with clinical and radiological features for diagnosis [4]. To illustrate this, an IgG4 test has a sensitivity of 76% and a specificity of 93% for AIP when levels greater than 140 mg/dL are detected. However, the most important role of IgG4 testing should be monitoring the response to medical treatment [1],[2],[6]. Elevated serum IgG4 levels are characteristics of AIP. However, mild elevations in serum IgG4 are seen in up to 10% of subjects without AIP including pancreatic cancer [4]. In type 1 AIP, extrapancreatic involvement is common, as the biliary tree, lacrimal and salivary glands, as well as the kidneys, retroperitoneum, pituitary, and prostate can be affected. Diagnosis is based on histological features: in type 1 AIP, lymphoplasmacytic sclerosing pancreatitis must be present, obliterative phlebitis, storiform fibrosis, and abundant (>10 cells/HPF) IgG4-positive cells can also be found [3],[4],[6].
Unlike in malignancies, AIP responds to steroids, and a trial with these can be performed if a malignancy is ruled out beforehand. A positive test shows rapid improvement in clinical and radiological conditions that must be confirmed after the first two weeks [1],[2]. The management of AIP is fundamentally medical, as treatment is based on long-term use of corticosteroids with dose adjustments. Nonetheless, on discontinuation of steroids, relapses can occur in up to 31% of patients with type 1 AIP and 9% of patients with type 2 AIP. Immunomodulator therapy has shown promise in patients with AIP, yet more research is needed [2],[3],[4].
In our case, a malignancy was considered as painless jaundice and weight loss manifested. Nonetheless, after a thorough examination, an AIP diagnosis was finally reached. Differentiation from pancreatic cancer remains challenging and misdiagnosis can still occur. A high index of suspicion is needed as AIP is infrequent and can mimic multiple pancreatic pathologies. Also, in a unique way, this case illustrates that any diagnosis must be fully investigated before taking a surgical or clinical decision.
CONCLUSION
Every action or plan taken on a patient is a risk. Making an accurate diagnosis is a priority on any pathology. When treating AIP differentiation from pancreatic carcinoma is vital as AIP can be treated with steroids and does not require surgery. High clinical awareness and close follow-up are critical in AIP. As relapse can occur, a multidisciplinary team of gastroenterologist, surgeons, and radiologists is necessary to adequately treat these kinds of patients. In a unique way this case also highlights that physicians must always consider these rare pathologies to minimize risks and prevent unnecessary life-threatening procedures.
REFERENCES
1.
Madhani K, Farrell JJ. Autoimmune pancreatitis: An Update on diagnosis and management. Gastroenterol Clin North Am 2016;45(1):29–43. [CrossRef]
[Pubmed]

2.
Majumder S, Takahashi N, Chari ST. Autoimmune pancreatitis. Dig Dis Sci 2017;62(7):1762–9. [CrossRef]
[Pubmed]
3.
Kwon JH, Kim JH, Kim SY, et al. Differentiating focal autoimmune pancreatitis and pancreatic ductal adenocarcinoma: Contrast-enhanced MRI with special emphasis on the arterial phase. Eur Radiol 2019;29(11):5763–71. [CrossRef]
[Pubmed]
4.
Ghazale A, Chari ST, Smyrk TC, et al. Value of serum IgG4 in the diagnosis of autoimmune pancreatitis and in distinguishing it from pancreatic cancer. Am J Gastroenterol 2007;102(8):1646–53.
[Pubmed]
5.
Erlij D, Ramos D, Montaña J, Kusnir P, Correa G, Neira O. IgG4-related disease, the new “great mimickerâ€: Report of one case. [Article in Spanish]. Rev Med Chil 2014;142(5):646–50. [CrossRef]
[Pubmed]
6.
Dickerson LD, Farooq A, Bano F, et al. Differentiation of autoimmune pancreatitis from pancreatic cancer remains challenging. World J Surg 2019;43(6):1604–11. [CrossRef]
[Pubmed]
7.
Del Chiaro M, Segersvard R, Lohr M, Verbeke C. Early detection and prevention of pancreatic cancer: Is it really possible today? World J Gastroenterol 2014;20(34):12118–31. [CrossRef]
[Pubmed]
8.
Chu LC, Goggins MG, Fishman EK. Diagnosis and detection of pancreatic cancer. Cancer J 2017;23(6):333–42. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Frans I Serpa - Substantial contributions to conception and design, Interpretation of data, Drafting the article, Final approval of the version to be published
Christian A Armijos - Substantial contributions to conception and design, Interpretation of data, Revising it critically for important intellectual content, Final approval of the version to be published
Marta L Cueva - Substantial contributions to conception and design, Drafting the article, Final approval of the version to be published
C Estefania Burbano - Interpretation of data, Drafting the article, Final approval of the version to be published
Gabriel A Molina - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Guaranter of SubmissionAll co-authors have made a substantial contribution to the design, data collection and analysis of the research and the drafting of the manuscript and have reviewed and accepted the contents of the manuscript prior to its submission by the corresponding author.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Copyright© 2020 Frans I Serpa et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



