 |
Case Report
Choledochal cyst in a young adult patient, a rare pathology that requires prompt and precise treatment
1 MD, PGY 4 General Surgery Resident, PUCE, Quito, Ecuador
2 MD, Attending Surgeon, Hospital Enrique Garces, Quito, Ecuador
3 MD, Attending Surgeon, Hospital Metropolitano, Quito, Ecuador
4 MD, General Practitioner, Hospital General Macas, Morona Santiago, Ecuador
5 MD, Attending Surgeon, Hospital General Macas, Morona Santiago, Ecuador
6 MD, Attending Surgeon, Department of General Surgery, Hospital IESS Quito Sur, Quito, Ecuador
Address correspondence to:
Gabriel A Molina
MD, Attending Surgeon, Department of General Surgery, Hospital IESS Quito Sur, Quito,
Ecuador
Message to Corresponding Author
Article ID: 100042S05JS2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Salazar JAD, Chimbo MRC, Arias HFD, Jaramillo PAP, Vélez XEM, Hidalgo CAQ, Fuentes G, Molina GA. Choledochal cyst in a young adult patient, a rare pathology that requires prompt and precise treatment. Edorium J Surg 2020;7:100042S05JS2020.ABSTRACT
Choledochal cysts are a rare congenital dilation of the biliary tract, they primarily affect females, young children, and are more prevalent in Asian individuals. Choledochal cysts are associated with recurrent episodes of biliary, pancreatic infections and malignant transformation. Complete excision of the choledochal cyst is the treatment of choice, therefore prompt diagnosis, timely surgery, and close follow-up are of paramount importance. We present the case of a 22-year-old female, who presented with cholestasis and abdominal pain. A Todani IA choledochal cyst was detected and successfully treated. On follow-ups she is doing well.
Keywords: Biliary tract, Choledochal cyst, Common bile duct
INTRODUCTION
Choledochal cysts are rare congenital anomalies of the bile ducts, more than 60% of them present during the first year of life and few cases appear in adulthood [1],[2]. Clinical presentation can be misleading as symptoms are nonspecific and can mimic many biliary or pancreatic conditions [1],[3]. Due to the high risk of malignant transformation, complete excision should always be considered [4]. We present the case of a young female patient with a Todani IA choledochal cyst. She was quickly diagnosed and successfully treated. On followups the patient is doing well.
CASE REPORT
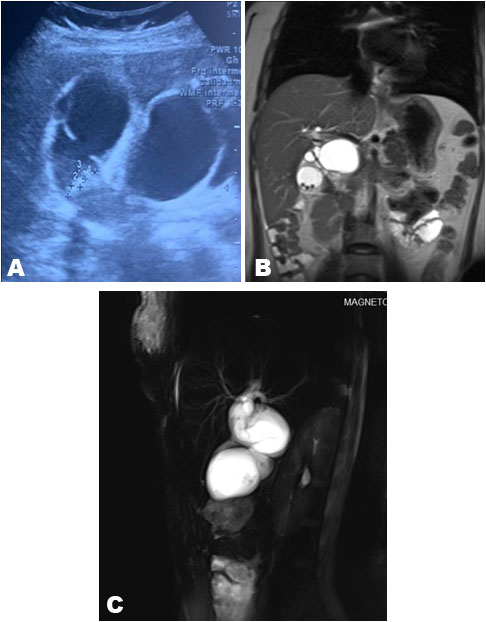
The patient was a 22-year-old female without past medical history. She presented to the emergency room with a 7-day history of upper abdominal pain, nausea, fever, and intermittent episodes of vomits. She noticed a yellowish tinge to the skin and the whites of the eye, 24 hours before her arrival. Thus, she was brought immediately by her family to the emergency room. Clinical examination revealed jaundice, abdominal tenderness, and a mass in her upper right abdomen. Complementary exams were requested; leukocytosis (16 × 109/L), neutrophilia (92%), and hyperbilirubinemia (7 mg/dL) were discovered. An abdominal echography unveiled a thin-walled gallbladder with gallstones and a 4 × 4 × 4.5 cm cystic lesion in the common bile duct (Figure 1A). Therefore, a magnetic resonance imaging (MRI) was requested exposing a Type IA choledochal cyst, the cyst measured 4 × 4 × 43 cm and comprised the entire common bile duct, also choledocholithiasis was found (Figure 1B and Figure C). The intrahepatic ducts were normal, and no masses or lymph nodes were discovered.
With these findings, surgery was decided. At laparotomy, radical resection of the cyst with reconstruction with a hepatic jejunostomy was planned. The bile duct was dissected, and the cyst was exposed, it extended at the top, 1 cm distal from the carina, to the intrapancreatic portion (Figure 2).
The cyst was dissected from the portal vein, the right and left hepatic ducts were identified, and the gallbladder was completely dissected. Clips were placed 0.5 cm from the top edge and the bottom edge of the cyst, and the lesion was completely removed. Following this, a Roux-en-Y hepaticojejunostomy was completed without complications.
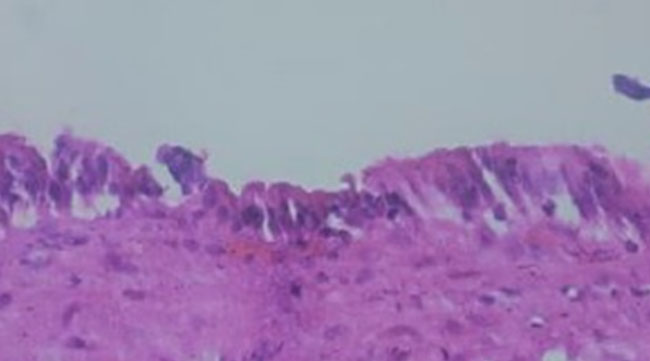
The pathology reported a choledochal cyst, without evidence of malignancy (Figure 3). Her postoperative course was uneventful, liquid diet was started on her second postoperative day and she was discharged without complications. On follow-ups, the patient is doing well.

DISCUSSION
Choledochal cysts are congenital cystic dilations of the biliary tract and were first described by Vater and Ezler in 1723 [1],[2]. They are rare lesions (1 in 100,000 individuals) with a greater predisposition in the Asian population, they predominantly appear in children (60%) and mostly on females [3]. As it was found in our patient.
Although the specific etiology is still under research, since 1969 when Babbit et al. first described the anomalous pancreaticobiliary duct union, it is believed that the reflux of pancreatic fluid into the biliary tree can contribute to the formation of the cysts [1],[3],[4]. Other theories include a weak bile duct wall, sustained intrabiliary pressure, sphincter of Oddi dysfunction, and distal obstruction of the common bile duct [2],[3].
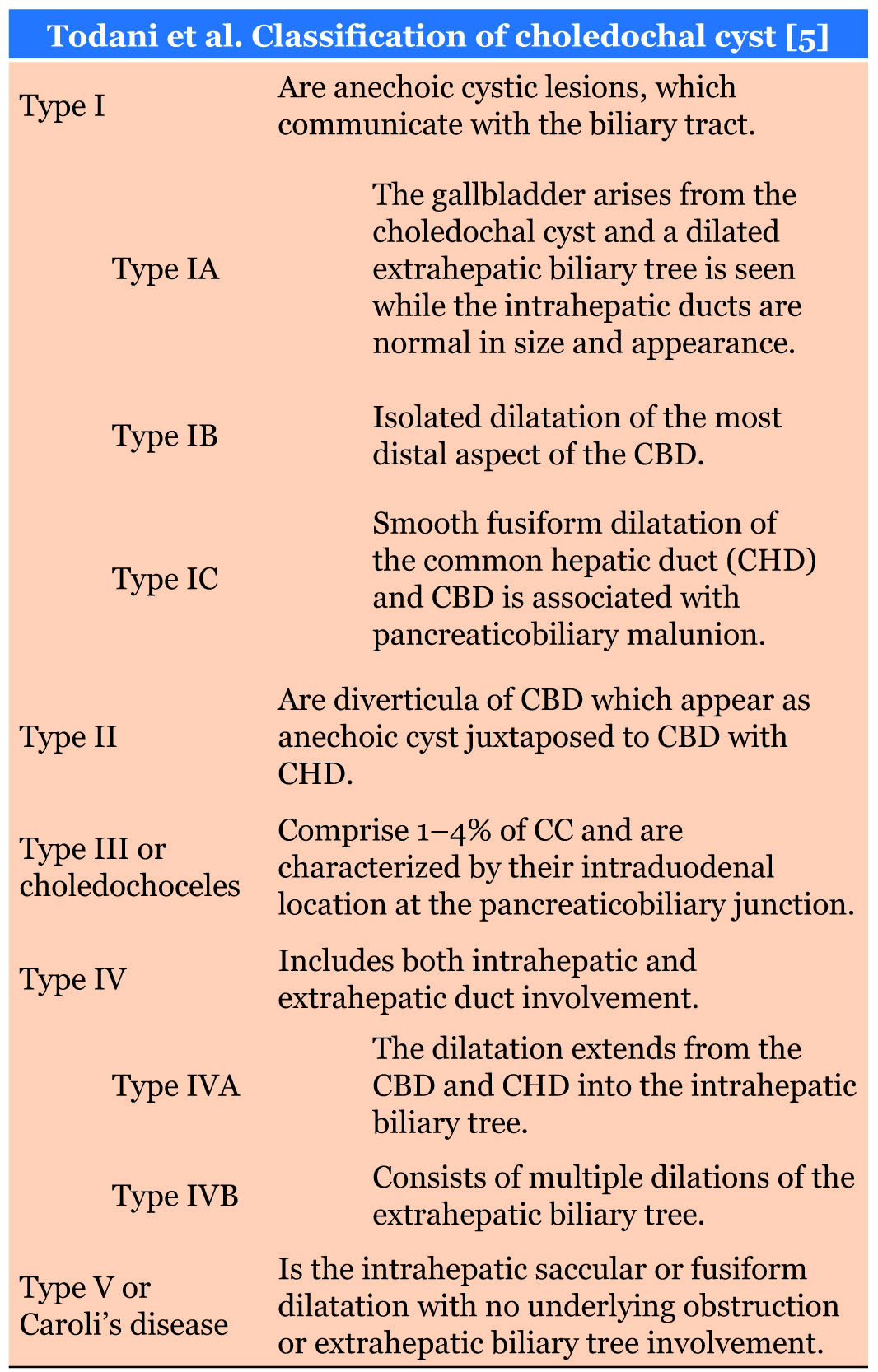
There are many classifications regarding choledochal cysts, nonetheless, the most widely accepted classification is the one by Todani et al. (Table 1) based on the site of the cyst [1],[6]. Five types of choledochal cyst are described and classified. Type I (80–90%), type II (2%), type III (1–4%), types IV and V (Caroli’s disease) [1],[2].
Type I cysts are usually anechoic lesions that communicate with the biliary tract, they can be further differentiated in three types [1],[3]. IA in which the extrahepatic biliary tree is dilated but the intrahepatic ducts are normal, IB contains mostly a normal extrahepatic hepatic biliary tree with an isolated dilatation on the distal common bile duct, and IC when there is a smooth fusiform dilatation of the common bile duct [4],[6]. Most patients experience upper abdominal pain and jaundice. Children may be asymptomatic or suffer from cholangitis [1],[7]. Adults usually present with infection complications, abdominal masses, or malignancy [4],[7]. In our case, the patient presented with cholangitis, and after timely treatment, the choledochal cyst was detected [7],[8]. Asymptomatic patients comprise 10–36% of the cases and are now more commonly detected with the use of cross-sectional imaging [1],[9]. Ultrasound, MRI, or endoscopic retrograde cholangiopancreatography (ERCP) can also aid in the diagnosis [1],[2],[10]. As it was found in our patient.
To prevent hepatic, pancreatic, or biliary consequences including recurrent episodes of cholangitis, pancreatitis, hepatic cirrhosis, or malignancy, complete cyst excision is recommended [1],[5],[11]. Malignancy is strongly associated with choledochal cysts (80–90% with type I or IVA), therefore, surgery should be performed once complications have been overcome [1],[4]. Complete excision of the cyst with biliary reconstruction is recommended due to the high risk of cholangiocarcinoma [8],[9]. For patients with types IV and V, liver transplantation may be the only means of eliminating the risk of cholangiocarcinoma [1],[10],[11]. Close follow-up is mandatory as the risk of subsequent biliary malignancy after surgery seems to be relatively high in the long term [1],[6].
In our case, after the cyst was detected, complete excision was achieved, and the patient completely recovered.
CONCLUSION
Choledochal cysts are a rare but treatable condition when a prompt diagnosis is made. High clinical suspicion, well-timed surgery, and close follow-up are of paramount importance in this rare disease. Surgeons should be highly prepared and trained to face these uncommon pathologies.
REFERENCES
1.
Ronnekleiv-Kelly SM, Soares KC, Ejaz A, Pawlik TM. Management of choledochal cysts. Curr Opin Gastroenterol 2016;32(3):225–31.
[Pubmed]

2.
Soares KC, Arnaoutakis DJ, Kamel I, et al. Choledochal cysts: Presentation, clinical differentiation, and management. J Am Coll Surg 2014;219(6):1167–80. [CrossRef]
[Pubmed]
3.
Edil BH, Cameron JL, Reddy S, et al. Choledochal cyst disease in children and adults: A 30-year single-institution experience. J Am Coll Surg 2008;206(5):1000–5. [CrossRef]
[Pubmed]
4.
Lee SE, Jang JY, Lee YJ, et al. Choledochal cyst and associated malignant tumors in adults: A multicenter survey in South Korea. Arch Surg 2011;146(10):1178–84. [CrossRef]
[Pubmed]
5.
Soares KC, Kim Y, Spolverato G, et al. Presentation and clinical outcomes of choledochal cysts in children and adults: A multi-institutional analysis. JAMA Surg 2015;150(6):577–84. [CrossRef]
[Pubmed]
6.
Ohashi T, Wakai T, Kubota M, et al. Risk of subsequent biliary malignancy in patients undergoing cyst excision for congenital choledochal cysts. J Gastroenterol Hepatol 2013;28(2):243–7. [CrossRef]
[Pubmed]
7.
Liu CL, Fan ST, Lo CM, Lam CM, Poo RT, Wong J. Choledochal cysts in adults. Arch Surg 2002;137(4):465–8. [CrossRef]
[Pubmed]
8.
Powell CS, Sawyers JL, Reynolds VH. Management of adult choledochal cysts. Ann Surg 1981;193(5):666–76. [CrossRef]
[Pubmed]
9.
Sela-Herman S, Scharschmidt BF. Choledochal cyst, a disease for all ages. Lancet 1996;347(9004):779. [CrossRef]
[Pubmed]
10.
Khandelwal C, Anand U, Kumar B, Priyadarshi RN. Diagnosis and management of choledochal cysts. Indian J Surg 2012;74(1):29–34. [CrossRef]
[Pubmed]
11.
Hamid R, Bhat NA, Ahmad M, Singh B. Choledochal Cyst (CDC). In: Neri V, editor. Gastrointestinal Surgery - New Technical Proposals. IntechOpen; 2018. [CrossRef]
SUPPORTING INFORMATION
Author Contributions
Jhony Alejandro Delgado Salazar - Substantial contributions to conception and design, Interpretation of data, Revising it critically for important intellectual content, Final approval of the version to be published
Mario Rafael Chaves Chimbo - Substantial contributions to conception and design, Interpretation of data, Drafting the article, Final approval of the version to be published
Harry Francisco Dorn Arias - Substantial contributions to conception and design, Revising it critically for important intellectual content, Final approval of the version to be published
Paola Alexandra Palacios Jaramillo - Acquisition of data, Interpretation of data, Drafting the article, Final approval of the version to be published
Xavier Eduardo Moreno Vélez - Substantial contributions to conception and design, Interpretation of data, Drafting the article, Final approval of the version to be published
Carlos Andrés Quinteros Hidalgo - Substantial contributions to conception and design, Acquisition of data, Drafting the article, Final approval of the version to be published
Germanico Fuentes - Substantial contributions to conception and design, Interpretation of data, Revising it critically for important intellectual content, Final approval of the version to be published
Gabriel A Molina - Substantial contributions to conception and design, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2020 Jhony Alejandro Delgado Salazar et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



