 |
Editorial
Release of intractable anastomotic stricture of the alimentary tract using a stenosis-cutting device
1 Senior Surgeon, Department of Surgery, Kumamoto General Hospital, Japan Community Health Care Organization (JCHO), Yatsushiro, Kumamoto, Japan
2 Chief, Department of Surgery, Kumamoto General Hospital, Japan Community Health Care Organization (JCHO), Yatsushiro, Kumamoto, Japan
3 Director, Kumamoto General Hospital, Japan Community Health Care Organization (JCHO), Yatsushiro, Kumamoto, Japan
Address correspondence to:
Shinya Shimada
Kumamoto General Hospital, Japan Community Health Care Organization (JCHO), 10-10 Tohricho, Yatsushiro, Kumamoto 866-8660,
Japan
Message to Corresponding Author
Article ID: 100053S05SI2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Ikeshima S, Horino K, Shimada S. Release of intractable anastomotic stricture of the alimentary tract using a stenosis-cutting device. Edorium J Surg 2021;8:100053S05SI2021.ABSTRACT
No Abstract
Keywords: Anastomosis, Esophagus, Rectum, STENO-CUTTER, Stricture
Editorial
The circular stapling of anastomosis of the alimentary tract is widely performed and regarded as a safe and quick technique. However, the frequent development of anastomotic strictures is a major postoperative complication of this procedure [1],[2]. Limited information is currently available on the complication of anastomotic strictures after the double stapling technique for low anterior resection of the rectum [3],[4]. On the other hand, in the reconstruction of the cervical esophagus using the cervical transposition of a jejunal segment, a major complication is the disruption and/or ischemic injury of the pharyngojejunal anastomosis or jejunal segment, leading to severe stricture [5],[6],[7].
Recent advances in fluoroscopic and endoscopic modalities have enabled us to perform effective, relatively safe, and minimally invasive procedures, such as fluoroscopically guided bougienage or endoscopic balloon dilation for acute, recurrent, or chronic strictures of the alimentary tract [8],[9]. Although good clinical outcomes have been achieved for accessible upper and lower gastrointestinal anastomotic strictures without disruption or ischemic injury, these techniques are not as effective for strictures caused by anastomotic disruption or ischemic injury. Since this type of stricture is generally severe and has a long narrow segment, it is intractable to dilatation and recurrence is common. Furthermore, refractory stricture of the alimentary tract causes severe pain in postoperative patients.
We developed a novel staple cutter for refractory anastomotic strictures [10],[11],[12]. We herein review this device, its clinical use and effects, as well as its advantages.
Stenosis-cutting device
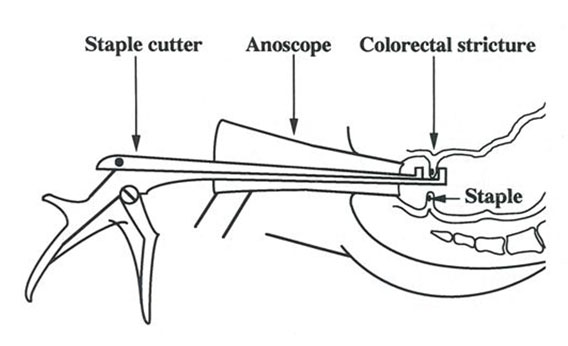
We developed a novel device and technique for stricture dilation after the circular stapling of anastomoses. The effects and advantages of this procedure using a staple cutter named STENO-CUTTER (M&M, Tokyo, Japan) for the treatment of strictures have been demonstrated [10]. As shown in Figure 1, STENO-CUTTER is a simple device that consists of two 3- or 5-mm sharp edges and a handle. The total lengths of the devices are 24.0, 30.5, and 33 cm, and the head is constructed to be as small as possible in order to pass anastomotic stenosis (width of 6 or 8 mm). Although the STENO-CUTTER was initially developed to split a circular stapler line in colorectal strictures, the device and technique may be applied to severe and recurrent strictures associated with anastomotic leakage, disruption, and/or ischemic injury [10],[11],[12].
Effects of stapling and stenosis cutting
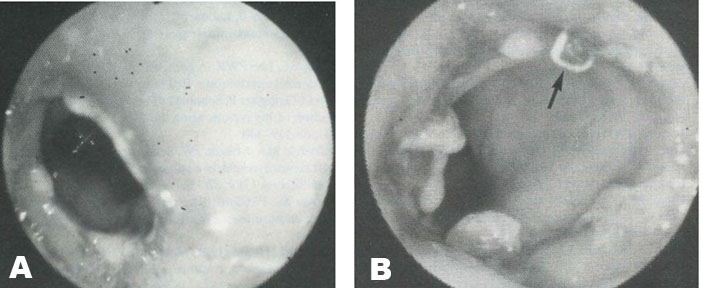
In strictures after colorectal anastomosis, using an anoscope with an electric light (diameter of 20 mm, length of 90 mm), two or three feasible sites were cut with the STENO-CUTTER under direct vision and digitally dilated without general anesthesia, as shown in Figure 2. In patients with very severe strictures with leakage and/or ischemic injury, fluoroscopically guided bougienage or endoscopic balloon dilatation of the anastomosis was required to pass the head of the cutter prior to the cutting procedure. In contrast to patients with short strictures without leakage and/or ischemic injury, multiple cuts were needed for the opposite two sites because the strictures consisted of firm fibrosis and formed a long narrow segment, as described above (generally three sites). 32 patients already underwent this treatment of cutting with the STENO-CUTTER, this procedure enabled us to obtain sufficient dilation of >20 mm in diameter relative to the diameter of the anoscope (Figure 3) in 28 (87.5%) of the 32 patients. Complications, such as perforation or significant bleeding, did not occur in any case. The symptom of frequent defecation before and after stenosis cutting was significantly attenuated after the treatment [11],[12].
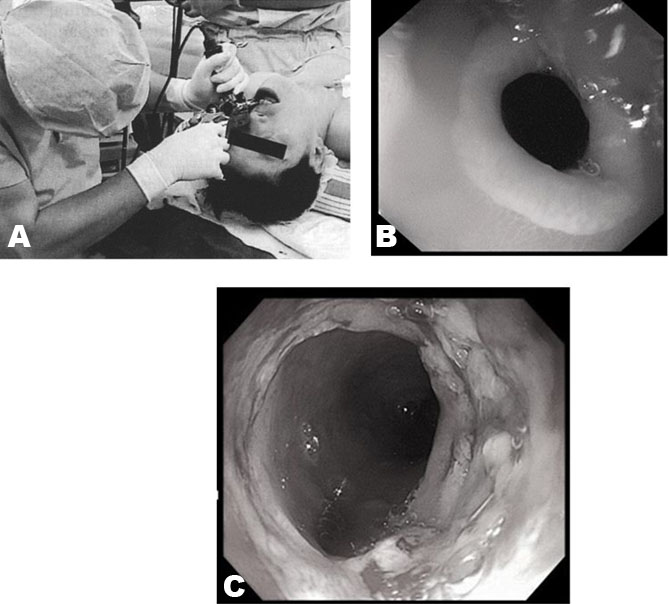
Regarding strictures of a pharyngojejunal anastomosis or jejunal segment with vascular anastomosis, with the patient under general anesthesia, a conventional rectal scope (length of 15 cm) was inserted in front of the stricture through the patient’s mouth, and the stricture was cut using the STENO-CUTTER under direct vision. The two parts of the stricture were cut in order to remove severe stenosis (Figure 4A). After cutting, a video endoscope was inserted to confirm dilation. The endoscope generally passed easily through the anastomosis [12].
We now perform a treatment that combines fluoroscopically guided bougienage or endoscopic balloon dilation after cutting with the STENO-CUTTER.
Between January 2015 and December 2019, seven patients with strictures of a pharyngojejunal anastomosis or esophagojejunostomy, a transpositioned jejunal segment with a vascular anastomosis after surgery for cervical esophageal cancer, underwent cutting with the STENO-CUTTER and endoscopic balloon dilation. This procedure achieved sufficient dilation in all seven patients (Figure 4B and Figure 4C). After dilation, the endoscope passed easily through the anastomosis. All patients underwent a gastroendoscopic examination every six months, with most not requiring redilation. The complete resolution of strictures has been maintained in the long term without the need for additional treatment.
Possible complications of the STENO-CUTTER are bleeding and perforation of the alimentary tract; however, substantial bleeding or perforation did not occur during or after cutting in any of the patients examined herein.

CONCLUSION
Cutting with the STENO-CUTTER is simple and easy under direct vision using a conventional anoscope or rectal scope. The intractable stricture of coloproctostomy for low anterior resection, pharyngojejunal anastomosis or esophagojejunostomy, and a transpositioned jejunal segment with a vascular anastomosis after surgery for cervical esophageal cancer are very successfully treated using the STENO-CUTTER. Complications, such as bleeding and perforation, did not occur. Therefore, the STENO-CUTTER is strongly recommended for the removal of strictures after alimentary tract anastomosis.
REFERENCES
1.
Ravitch MM, Steinchen FM. A stapling instrument for end-to-end inverting anastomoses in gastrointestinal tract. Ann Surg 1979;189(6):791–7.
[Pubmed]

2.
Cade D, Gallagher P, Schofield PF, Turner L. Complications of anterior resection of the rectum using the EEA stapling device. Br J Surg 1981;68(5):339–40. [CrossRef]
[Pubmed]
3.
Knight CD, Griffen FD. An improved technique for low anterior resection of the rectum using the EEA stapler. Surgery 1980;88(5):710–4.
[Pubmed]
4.
Varma JS, Chan AC, Li MK, Li AK. Low anterior resection of the rectum using a double stapling technique. Br J Surg 1990;77(8):888–90. [CrossRef]
[Pubmed]
5.
Kasai M, Nishihara T. Reconstruction using pedicled jejunal segments after resection for carcinoma of cervical esophagus. Surg Gynecol Obstet 1986;163(6):145–52.
[Pubmed]
6.
Urayama H, Ohtake H, Ohmura K, Watanabe Y. Pharyngoesophageal reconstruction with the use of vascular anastomoses: Operative modification and long-term prognosis. J Thorac Cardiovasc Surg 1997;113(6):975–81. [CrossRef]
[Pubmed]
7.
Mansour KA, Bryan FC, Carlson GW. Bowel interposition for esophageal replacement: Twenty-five-year experience. Ann Thorac Surg 1997;64(3):752–6. [CrossRef]
[Pubmed]
8.
Marshall JB, Afridi SA, King PD, Barthel JS, Butt JH. Esophageal dilation with polyvinyl (American) dilators over a marked guidewire: Practice and safety at one center over a 5-yr period. Am J Gastroenterol 1996;91(8):1503–6.
[Pubmed]
9.
Hagiwara A, Togawa T, Yamasaki J, Shirasu M, Sakakura C, Yamagishi H. Endoscopic incision and balloon dilatation for cicatricial anastomotic strictures. Hepatogastroenterology 1999;46(26):997–9.
[Pubmed]
10.
Shimada S, Matsuda M, Uno K, Matsuzaki H, Murakami S, Ogawa M. A new device for the treatment of coloproctostomic stricture after double stapling anastomoses. Ann Surg 1996;224(5):603–8. [CrossRef]
[Pubmed]
11.
Shimada S, Yagi Y, Yamamoto K, Matsuda M, Baba H. Novel treatment of intractable rectal strictures associated with anastomotic leakage using a stenosis-cutting device. Int Surg 2007;92:82–8.
[Pubmed]
12.
Shimada S, Honmyo U, Hayashi N, Matsuda M, Ogawa M. Successful new treatment for intractable cervical esophageal stenosis of a jejunal segment transpositioned with a vascular anastomosis: Report of a case. Surg Today 2002;32(11):996–9. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Satoshi Ikeshima - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Kei Horino - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Shinya Shimada - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Satoshi Ikeshima et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



