 |
Case Report
Intestinal obstruction, pneumoperitoneum, and colon carcinoma within an inguinoscrotal hernia
1 PhD, Medical Area Specialist in General Surgery, Department of General Surgery, Hospital El Escorial, Francisco de Vitoria University (UFV), San Lorenzo de El Escorial, Madrid, Spain
2 PhD, Chief of Department, Department of General Surgery, Hospital El Escorial, Francisco de Vitoria University (UFV), San Lorenzo de El Escorial, Madrid, Spain
3 MD, Medical Area Specialist in General Surgery, Department of General Surgery, Hospital El Escorial, Francisco de Vitoria University (UFV), San Lorenzo de El Escorial, Madrid, Spain
Address correspondence to:
Sonia Morales Artero
Hospital El Escorial, Road M-600 Guadarrama to San Lorenzo de El Escorial, Km 6.255, 28200 San Lorenzo de El Escorial, Madrid,
Spain
Message to Corresponding Author
Article ID: 100055S05MC2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
de Castro M, Larraz E, Morales S, Cereceda P, Martin L, Calvo M. Intestinal obstruction, pneumoperitoneum, and colon carcinoma within an inguinoscrotal hernia. Edorium J Surg 2021;8:100055S05MC2021.ABSTRACT
Introduction: Inguinal hernias with neoplastic contents in the sac are extremely rare.
Case Report: We present a case of intestinal obstruction due to a sigmoid colon carcinoma hosted in an incarcerated left inguinal hernia, with cecum perforation. The computed tomography (CT) scan demonstrated pneumoperitoneum. Surgical treatment consisted in subtotal colectomy with protective ileostomy.
Conclusion: Complicated colon neoplasms included in hernia sacs require tailored treatment, depending on the patient’s condition and related morbidity.
Keywords: Colon carcinoma, Inguinal hernia, Intestinal obstruction, Pneumoperitoneum, Strangulation
INTRODUCTION
Colonic neoplasms included in hernia sacs are uncommon. Complicated cases, with bowel obstruction due to incarceration of the hernia contents, are even more rare. The first description of a colon carcinoma located in a hernia sac was made by Fieber and Wolstenholme in 1955 [1]. We report the case of a patient with intestinal obstruction due to an incarcerated inguinoscrotal hernia containing an obstructive sigmoid carcinoma, and pneumoperitoneum due to a cecum perforation.
CASE REPORT
A 79-year-old man presented to the emergency department with a 3-day-history of abdominal pain and distension without emission of gas or stool. He reported no fever. He had past medical history of left inguinal hernia, hypertension, and chronic ischemic heart disease, with controlled atrial fibrillation. On physical exam, the abdomen showed distension, pain on deep palpation and guarding. A giant non-reducible inguinoscrotal hernia was identified (Figure 1).
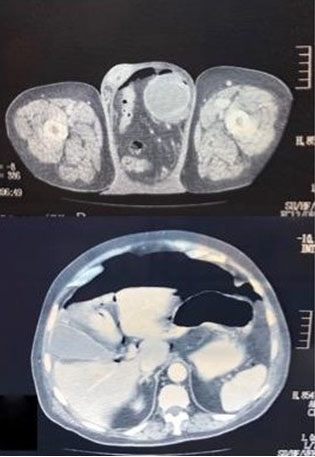
Computed tomography scan showed pneumoperitoneum with a small amount of free fluid, a severe dilation of the colon and a giant left inguinoscrotal hernia (Figure 2).
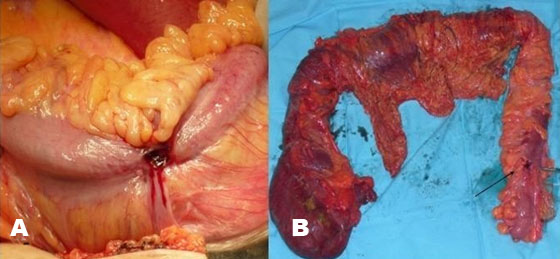
The patient underwent surgical treatment. A midline supra-infra-umbilical laparotomy was performed. A small perforation was identified in the cecum, which was severely dilated, as was the rest of the colon. The sigmoid was found passing through an inguinal ring and included in the sac of a giant left inguinoscrotal hernia. After reducing it back to the abdominal cavity, a stenotic sigmoid mass of malignant appearance was found (Figure 3A and Figure 3B). Subtotal colectomy with ileo-rectal anastomosis was performed, leaving a lateral protective ileostomy. The hernia ring was repaired with suture from the inside of the peritoneal cavity. The patient developed postoperative pneumonia with a favorable course on antibiotics and physiotherapy. Pathological exam revealed a colorectal stage II carcinoma (T3N0M0).

DISCUSSION
Simultaneous finding of an inguinal hernia and a colorectal carcinoma is a rare event; it represents less than 0.5% of incarcerated hernias [2].
Lejar [3] classifies hernia contents as saccular or extrasaccular, depending on their location. Saccular contents include primary peritoneal tumors, such as mesothelioma, or peritoneal metastases; intrasaccular usually corresponds to intestinal tumors. Some publications report perforated colonic tumors hosted inside an inguinal hernia sac, which severely complicate the patient’s prognosis [4],[5],[6]. Cases of colon perforation in ventral hernias have also been reported [7],[8].
In the present case, we found an incarcerated hernia with a sigmoid colon carcinoma hosted in the sac. There was no perforation inside the sac. However, there was bowel obstruction and a micro-perforation in the cecum due to hyper-pressure. Clinical suspicion about neoplasia in a hernia sac must be taken into account in patients older than 70 years, who suffer from large long-lasting hernias [9]. Computed tomography scan was essential for diagnosis in our case, as it demonstrated both colonic obstruction and pneumoperitoneum.
Surgical approach in these complicated cases of bowel obstruction and inguinal hernia remains controversial [10]. We decided an open laparotomy because of the presence of pneumoperitoneum. This allowed us to clearly identify a cecum micro-perforation, responsible for the pneumoperitoneum, and to perform an oncological colonic resection, namely subtotal colectomy with lateral protective ileostomy. We did not perform an anterior repair of the inguinal hernia to avoid surgical wound contamination, as the surgery was considered as Class III. We decided to close the hernia ring from the abdominal side. Thus, we considered not to use prosthetic material for reinforcement. In uncomplicated cases, surgical approach may vary from a wide transverse laparotomy [5] to initial inguinal approach and subsequent laparotomy if needed [9]. There are some reported cases of laparoscopic approach to an incarcerated hernia containing a cecum carcinoma inside the sac [11].
CONCLUSION
In conclusion, colonic carcinomas included in hernia sacs with associated complications such as the ones we describe in this case are very rare. Surgical approach is variable and must be tailored to the patient.
REFERENCES
1.
Fieber SS, Wolstenholme JT. Primary tumours in inguinal hernial sacs. AMA Arch Surg 1955;71(2):254–6. [CrossRef]
[Pubmed]

2.
Boormans JL, Hesp WLEM, Teune TM, Plaisier PW. Carcinoma of the sigmoid presenting as a right inguinal hernia. Hernia 2006;10(1):93–6. [CrossRef]
[Pubmed]
3.
Lejar J. Neoplasmes herniaires et peri-herniaires. Gaz Hosp 1889;62:801–11.
4.
Kouraklis G, Kouskous E, Glinavou A, Raftopoulos J, Karatzas G. Perforated carcinoma of the sigmoid colon in an incarcerated inguinal hernia: Report of a case. Surg Today 2003;33(9):707–8. [CrossRef]
[Pubmed]
5.
Tan GY, Taylor G, Ahmed T. Perforated sigmoid colon carcinoma in an irreductible inguinoscrotal hernia. Ann R Coll Surg Engl 2013;95(7):125–6. [CrossRef]
[Pubmed]
6.
Kulasegaran S, Fernando M, Fraser-Jones B, Hammodat H. Perforated sigmoid colon carcinoma within a left inguinal hernia with associated necrotising infection. NZ Med J 2016;129(1431):93–5.
[Pubmed]
7.
Grelotti DJ, Riall TS, Williams CG. A palpable, obstructing carcinoma of the colon incarcerated within a large ventral hernia. J Gastronintest Surg 2006;10(7):1092–4. [CrossRef]
[Pubmed]
8.
Lapropoulos P, Liarmakopoulos E, Markakis C, et al. Colon cancer perforation presenting as a strangulating ventral hernia. Case Rep Oncol 2012;5(1):17–21. [CrossRef]
[Pubmed]
9.
Slater R, Amatya U, Shorthouse AJ. Colonic carcinoma presenting as a strangulated inguinal hernia: Report of two cases and review of the literatura. Tech Coloproctol 2008;12(3):255–8. [CrossRef]
[Pubmed]
10.
Ruiz-Tovar J, Ripalda E, Beni R, Nistal J, Monroy C, Carda P. Carcinoma of the sigmoid colon in an incarcerated inguinal hernia. Can J Surg 2009;52(2):E31–2.
[Pubmed]
11.
Pernazza G, Monsellato I, Alfano G, et al. Laparoscopic treatment of a carcinoma of the cecum incarcerated in a right groin hernia: Report of a case. Surg Today 2011;41(3):422–5. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Mar de Castro - Substantial contributions to conception and design, Acquisition of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Elena Larraz - Substantial contributions to conception and design, Analysis of data, Interpretation of data, Revising it critically for important intellectual content, Final approval of the version to be published
Sonia Morales Artero - Substantial contributions to conception and design, Acquisition of data, Drafting the article, Final approval of the version to be published
Pablo Cereceda - Substantial contributions to conception and design, Revising it critically for important intellectual content, Final approval of the version to be published
Libertad Martin - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Montserrat Calvo - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Mar de Castro et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



