 |
Case Report
Laparoscopic approach to Amyand hernia: A case report
1 Attending Surgeon, MD, Department of General Surgery at Hospital IESS Quito Sur Quito-Ecuador, Ecuador
2 Resident, MD, Department of General Surgery at Hospital IESS Quito Sur, Ecuador
3 Intern, Department of General Surgery at Hospital IESS Quito Sur, Ecuador
4 MD, Attending Surgeon, Universidad San Francisco de Quito (USFQ), Department of General Surgery at Hospital IESS Quito Sur Quito-Ecuador, Ecuador
Address correspondence to:
Gabriel A Molina
MD, Attending Surgeon, Department of General Surgery at Hospital IESS Quito Sur Quito-Ecuador,
Ecuador
Message to Corresponding Author
Article ID: 100049S05AA2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Ayala AV, Dávalos M, Aldaz JC, Lara AG, Ulloa MEC, Molina GA. Laparoscopic approach to Amyand hernia: A case report. Edorium J Surg 2020;7:100049S05AA2020.ABSTRACT
Introduction: Amyand’s hernia is an inguinal hernia containing the vermiform appendix. The herniated appendix can be inflamed during this stage. This rare inguinal hernia presentation is named after Claudius Amyand, the first surgeon to record an appendectomy. It is a rare event in which symptoms and signs are usually not obvious, leading to misdiagnosis, delay in treatment, and higher complication rates. Laparoscopy has become an invaluable tool for physicians, as it can accurately diagnose and treat unexpected pathologies, such as Amyand’s hernia in an emergency setting.
Case Report: We present the case of a 31-year-old male patient with acute abdominal pain. After clinical examination, surgery was required, and an Amyand’s hernia was discovered. The laparoscopic approach successfully treated this hernia without surgical site infection or complications.
Conclusion: Amyand’s hernia is an extremely rare presentation of an inguinal hernia. Due to its rare presentations and low incidence, it can easily be missed, leading to troublesome complications.
Keywords: Amyand's hernia, Inguinal hernia, Laparoscopic surgery
INTRODUCTION
Amyand’s hernia is defined as the presence of the vermiform appendix within an inguinal hernia sac [1],[2]. It is an extremely rare pathology (1% of all inguinal hernias) that can lead to troublesome complications if it is misdiagnosed [3],[4]. Open appendectomy and hernia repair were the mainstay treatment of this rare condition. However, with the advent of laparoscopic surgery, a less invasive procedure, we can provide more significant advantages to our patients [1],[5]. We report the case of a 31-year-old male patient. He presented with acute abdominal pain, and laparoscopic surgery was needed to treat him. Amyand’s hernia was detected and successfully treated.
CASE REPORT
We present the case of a 31-year-old male without past medical history. He presented to the emergency room with an 18-hour history of acute abdominal pain, nausea, and anorexia. On clinical examination, he was tachycardic (117), febrile (38°C) and with a blood pressure of 130/65. Severe pain on touch was detected on his lower abdomen. His pain was not migratory or colicky, although there was no tenderness or percussion pain over McBurney’s point. On groins inspection, no masses, lumps, or swellings were detected. Complementary exams, including complete blood count and abdominal echography, were normal. Thus, he was admitted for close surveillance. A computed tomography (CT) was considered, nonetheless as his pain persisted, hence, surgery was decided.
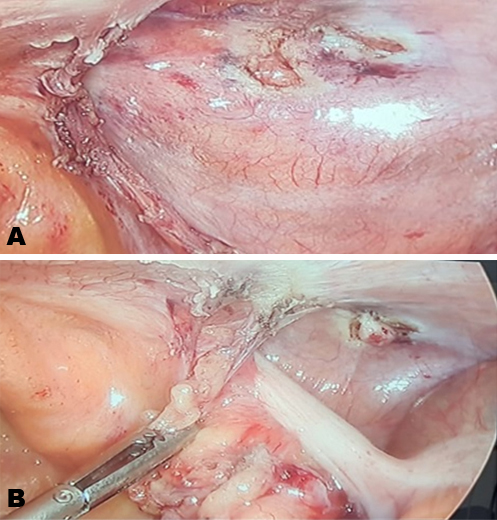
At laparoscopy, a 3 × 2 cm right-sided indirect inguinal hernia was discovered. The hernia sac was covered with the cecum and small bowel (Figure 1A). After blunt dissection to separate the bowel from the hernia sac, the vermiform appendix was found within the hernia sac (Figure 1B). After slightly dissecting the hernia sac, the appendix was removed without complications. The appendix measured 0.3 × 6 cm and was completely normal without signs of congestion or perforation.
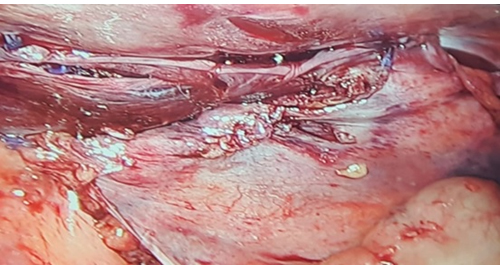
From there, dissection continued, and the hernia sac was grasped and released from the transverse fascia, and dissection of the extraperitoneal space was completed. A 10 × 15 cm polypropylene mesh was placed and secured with absorbable tacks. Afterward, the free peritoneal edges were grasped, brought up, and secured using tacks (Figure 2).
After this procedure, the appendix was re-assessed, and due to his clinical picture, and since the appendix was found within the hernia sac, an incidental appendectomy was decided. His postoperative course was uneventful. Sips of liquids were initiated on his first postoperative day and then after followed by full diet. He was discharged without complications on his second postoperative day without any pain and remained well on close follow-ups. He resumed full activity 3 months after surgery.
Pathology reported lymphoid hyperplasia with slight neutrophilic infiltration. Three months after surgery, he was completely asymptomatic and is doing well.
DISCUSSION
There are two sporadic events in which the vermiform appendix, inflamed or not, is discovered within the inguinal (Amyand) or femoral canal (de Garengeot). These hernias are named after Dr. Claudius Amyand and Dr. Croissant de Garengeot, the first physicians who described these conditions in 1736 and 1731 [1],[2],[3]. Amyand’s hernias occur in 0.4–0.6% of all inguinal hernias, and the presence of appendicitis within an Amyand’s hernia accounts for 0.1% of all appendicitis [1],[2]. These hernias are usually more common in children due to the patency of processus vaginalis in the pediatric population [1],[4]. Preoperative diagnosis is generally tricky as their abdominal exam, physical signs, lab results, and imaging are not always helpful [3]. Symptoms are usually non-specific and include sudden onset epigastric or periumbilical pain, tenderness, or even mass in the inguinal region, mimicking a hernia [1],[4],[5]. Computed tomography (CT) can aid in the diagnosis; however, since appendicitis and inguinal hernias are usually diagnosed clinically, it is rarely ordered on a regular basis and only use to rule out a more severe pathology [2],[6].
In our case, the patient presented with acute abdominal pain, and since the pain persisted, laparoscopic surgery was decided. Most cases are rarely diagnosed preoperatively, and many cases are diagnosed during surgery [2],[3]; as it happened to our patient. The herniated appendix can be normal, acutely inflamed, or perforated, and its treatment can be based on the Losanoff and Basson classification [3],[7],[8]. The hernia defect should always be repaired unless there are severe complications. The use of meshes in a contaminated environment is usually contraindicated due to the high risk of infection and should be avoided when the appendix is compromised [1],[9],[10]. Mortality from Amyand’s hernia range from 14% to 30%, and wound infection rates can be as high as 50%, mostly due to the abdominal sepsis that can happen if the appendix perforates[3],[11].
There is still no agreement in the literature concerning the best course of action in treating the appendix in Amyand’s hernia, while there are many reviews which argue that appendectomy should only be performed if the appendix is inflamed, others support appendectomy to avoid future complications. Nonetheless, the decision to remove the appendix will remain on the surgeon [1],[4],[6],[12].
As the appendix in our patient was found within the hernia sac and to prevent an appendectomy later, it was removed without complications despite its normal appearance. Although open approaches have been considered the usual treatment of Amyand’s hernias, the laparoscopic approach has proved useful when treating inguinal hernias [5],[6]. In 1999, Vermillion et al. were the first surgeons to prove that laparoscopy can be useful in Amyand’s hernias, as it can help identify unexpected pathologies in an emergency setting. It can provide a view of the hernia contents, successfully reduce the hernia, and perform a mesh repair if needed [4],[7],[8],[9].
CONCLUSION
Amyand’s hernia is an extremely rare presentation of an inguinal hernia. Due to its rare presentations and low incidence, it can easily be missed, leading to troublesome complications. High clinical awareness is necessary to provide prompt decisions and accurately treat this rare and unexpected pathology.
REFERENCES
1.
Schaaf KA, Melnychuk EM, Ellison, RD, Snover AJ. Two rare cases of appendicitis: Amyand's hernia and de Garengeot's hernia. Case Rep Emerg Med 2019;2019:6759206. [CrossRef]
[Pubmed]

2.
Milanchi S, Allins AD. Amyand's hernia: History, imaging, and management. Hernia 2008;12(3):321–2. [CrossRef]
[Pubmed]
3.
Shaban Y, Elkbuli A, McKenney M, Boneva D. Amyand's hernia: A case report and review of the literature. Int J Surg Case Rep 2018;47:92–6. [CrossRef]
[Pubmed]
4.
Ivanschuk G, Cesmebasi A, Sorenson EP, Blaak C, Loukas M, Tubbs SR. Amyand's hernia: A review. Med Sci Monit 2014;20:140–6. [CrossRef]
[Pubmed]
5.
Han SH, Li MY, Lai HF. A total laparoscopic treatment strategy for Amyand’s hernia complicated with appendicitis: A case report. Int J Surg Case Rep 2019;59:11–4. [CrossRef]
[Pubmed]
6.
Akaishi R, Nishimura R, Naoshima K, Miyazaki S. Amyand's hernia complicated with appendix perforation treated by two-stage surgery consisting of laparoscopic appendectomy followed by elective inguinal hernioplasty: A case report. Int J Surg Case Rep 2018;47:11–3. [CrossRef]
[Pubmed]
7.
MacArthur F, Dhabuwala A. Amyand's hernia: A hybrid laparoscopic and open approach. Hernia 2015;19(6):991–4. [CrossRef]
[Pubmed]
8.
Rehman MR, Panteli C, Tsang T. Laparoscopic repair of Amyand’s hernia in an 8-week-old infant. Hernia 2010;14(4):443–5. [CrossRef]
[Pubmed]
9.
Patoulias D, Kalogirou M, Patoulias I. Amyand's hernia: An up-to-date review of the literature. Acta Medica (Hradec Kralove) 2017;60(3):131–4. [CrossRef]
[Pubmed]
10.
Mebis W, Hoste P, Jager T. Amyand's hernia. J Belg Soc Radiol 2018;102(1):8. [CrossRef]
[Pubmed]
11.
Nieto Morales ML, El Khatib Ghzal Y, Santana Medina E. Amyand hernia. [Article in Spanish]. Cir Esp 2019;97(7):408. [CrossRef]
[Pubmed]
12.
Maternini M, Gabrielli F, Pecora N, Riggio V, Chiarelli M, Guttadauro A. Amyand hernia in an elderly patient. Ann Ital Chir 2018;7:S2239253X18028475.
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Andres V Ayala - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Macarena Dávalos - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Juan C Aldaz - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
A Gabriela Lara - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
María E Chávez Ulloa - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Gabriel A Molina - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2020 Andres V Ayala et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



