 |
Case Report
Pneumocephalus as complication from hyperbaric oxygen treatment
1 MD, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, Canada
2 MD, Associate Clinical Professor, Department of Surgery, University of Alberta, Edmonton, Alberta, Canada
Address correspondence to:
Lily Xiao Jing Sun
Edmonton, Alberta,
Canada
Message to Corresponding Author
Article ID: 100052S05LS2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Sun LXJ, Nataraj A. Pneumocephalus as complication from hyperbaric oxygen treatment. Edorium J Surg 2021;8:100052S05LS2021.ABSTRACT
Introduction:
Hyperbaric oxygen treatment (HBOT) is a therapy in which a patient breathes 100% oxygen intermittently while inside a treatment chamber at a pressure higher than at sea level. Barotrauma is the most common cause of side effects with HBOT. In this case report, we discuss the rare presentation of pneumocephalus following HBOT.
Case Report:
The patient is a 32-year-old woman with congenital hydrocephalus and an extensive history of shunt revisions, as well as a third ventriculostomy. The patient received two weeks of HBOT given her history of impaired wound healing and continuation of poor skin healing after a shunt revision surgery. This is the first report of pneumoventricle in the context of a non-healing ventriculoperitoneal (VP) shunt wound as a complication of HBOT.
Conclusion:
Although pneumocephalus after HBOT is a very rare complication, careful evaluation of the patient is needed prior to initiating HBOT. Increased awareness of this potential complication of HBOT can aid in the decision-making of whether to expose patients with non-healing VP shunt incisions to this therapy.
Keywords: Hyperbaric oxygen, Pneumocephalus, Ventriculoperitoneal shunt
INTRODUCTION
Hyperbaric oxygen treatment (HBOT) is a therapy in which a patient breathes 100% oxygen intermittently while inside a treatment chamber at a pressure higher than at sea level pressure (i.e., 0.1 atm) [1]. Indications of HBOT include carbon monoxide poisoning, decompression sickness, arterial gas embolism, radiation-induced tissue injury, acute traumatic ischemic injury, compromised skin grafts and flaps, anemia due to exceptional blood loss, thermal burns, clostridial myonecrosis, necrotizing fasciitis, and refractory osteomyelitis [2]. Ischemia is the most common cause of non-healing infected wounds [3]. Ischemia not only leads to hypoxia but also compromises antibiotic delivery [4]. Primary effects of hyperbaric oxygen treatment are the result of increased tissue oxygen partial pressure. Secondary effects are the result of a controlled oxidative stress producing reactive oxygen species and reactive nitrogen species involved in wound healing, improved leukocyte function and neovascularization [5].
The most common side effects of HBOT is barotrauma explained by pressure equalization problems causing middle ear pain, tooth pain, and cranial/paranasal sinus pain [6]. Other side effects include cranial nervous system oxygen toxicity seizure, hyperoxic myopia, cataracts, pulmonary edema, increase in blood pressure, decrease in pulmonary function, and risk of air trapping in patients with asthma or chronic obstructive pulmonary disease (COPD) [5]. Here, we discuss the rare presentation of pneumocephalus following HBOT for treatment of recurrent postoperative wound infection.
CASE REPORT
The patient is a 32-year-old woman with congenital hydrocephalus and an extensive history of shunt revisions, as well as a third ventriculostomy. Most were obstructions complicated by long-standing non-healing wounds postoperatively. She had a recurrent history of wound dehiscence and leaking of pus over the incision line as well as wound break down exposing the ventriculoperitoneal (VP) shunt and valve. In the past, one month of HBOT had been used for a non-healing VP shunt wound with some success. Her other relevant past medical history includes epilepsy treated with frontal lobe resection and left temporal lobectomy, complete heart block, and postoperative infections including multiple pacemaker infections.
Three months after receiving antibiotics for right parietotemporal osteomyelitis, the patient presented with acute confusion, fever, and headache. Bilateral shunts were removed and a left posterior external ventricular drain (EVD) was inserted after a VP shunt tap showed infection with Escherichia coli. After removal of the EVD, the patient developed symptoms of increased intracranial pressure (ICP). A left frontal EVD was then inserted and ICP was estimated to be 30 cm H2O. One week later, a VP shunt was inserted through the right frontal area. Because of persistent ventricular dilation, on postoperative day 8 of the VP shunt insertion, revision of the shunt with partial septum pellucidum ostomy was performed using ventriculoscopic guidance. Given her history of impaired wound healing and continuation of poor skin healing, HBOT was started and continued after this operation for two weeks.
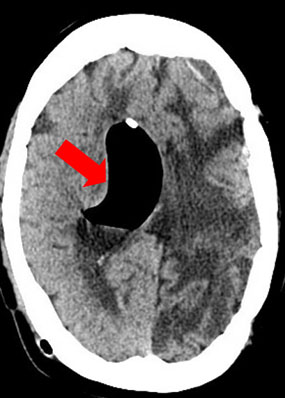
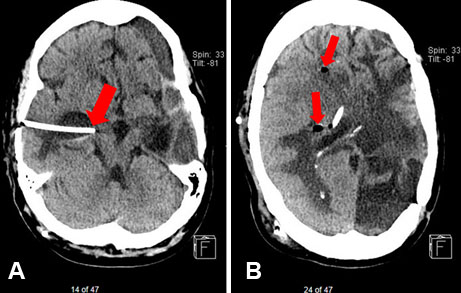
The patient was neurologically stable for the next two months until she presented with decreased level of consciousness (LOC), headache, and recurrent episodes of clonic and myoclonic jerking of the upper extremities. There was a significant amount of air distending the right lateral ventricle with midline shift and a hemorrhage involving the left frontal temporal region (Figure 1). The initial shunt tap drew 15 mL of air and the ventricles decreased in size. The shunt was later tapped two more times and no organisms grew. Air in the right ventricle resolved over the next 10 days, but the ventricles kept on dilating requiring a VP shunt revision. After this revision and over the following week, there were two more shunt obstructions requiring revisions. After a new VP shunt system was inserted, one day postoperatively, the right temporal horn became trapped (Figure 2). A right temporal shunt catheter was inserted for the isolated right temporal horn hydrocephalus for decompression (Figure 3A and Figure 3B).
One week after the insertion of the temporal shunt catheter, the patient deteriorated neurologically to a Glasgow Coma Scale (GCS) of 6, associated with another slight enlargement of the temporal horn of the right lateral ventricle. Both the right-sided frontal and temporal ventricular shunt were externalized, and the patient improved. While the drains were clamped awaiting further shunt revision, there was no subsequent increase in ventricular size. The patient’s shunt was removed 12 days after the shunt was externalized and clamped. The patient was discharged after three days of the removal of the shunt. Despite clamping and removing the externalized shunts, her ventricles did not enlarge, nor did she develop symptoms. Ultimately, she stayed stable and was no longer shunt dependent. At four-year follow-up, the patient’s symptoms remained stable with no shunt. In summary, the patient had nine shunt revisions before presentation and seven shunt revisions after presentation.

DISCUSSION
The large amount of air distending the right ventricle with midline shift causing decreased LOC and seizure is a possible complication from HBOT. Tension pneumocephalus has been described in the past as a rare complication from HBOT, but this is the first report of air becoming entrapped in the ventricular system as a possible consequence of HBOT of which we are aware [7],[8]. The mechanism is thought to be related to the cyclical pressure change with initiation and completion of each HBOT session [7]. While undergoing HBOT, the patient is in a high-pressure environment creating a negative pressure in the intracranial space causing air to enter the intracranial space through dural and skull defects. Once the patient returns back to atmospheric pressure, intracranial air volume expands to push out cerebrospinal fluid (CSF) through the structural defects [7]. A greater negative pressure will develop intracranially in subsequent sessions of HBOT as the existing intracranial air is compressed during HBOT allowing more air to enter [7]. The cycle repeats itself leading to the buildup of air intracranially. Given the patient’s history of multiple shunt insertions and poor wound healing, air likely has reached the ventricle through the tract created by the catheter and postoperative wounds [9].
Another possible but less likely cause of pneumocephalus in this patient includes CSF leak from her multiple neurosurgical operations. Presence of a cranio-dural defect and diversion of CSF are the two requirements for pneumocephalus to occur [10]. Infection with gas-producing organisms can also cause pneumocephalus but unlikely to be the culprit for this patient. No organisms grew from the shunt tap along with normal CSF protein, glucose, and low white blood cell count. In addition, no organisms grew on the catheter specimen. Blood work and blood culture also did not show any signs of infection for this patient during the large accumulation of ventricular air.
Entrapment of the right temporal horn is another interesting presentation. Isolated dilatation of the temporal horn is an extremely rare pathologic condition [11]. There have only been 72 reported cases of temporal horn entrapment from 1947 to 2017 [12]. Possible causes include central nervous system infection, hemorrhage, intra- and extra-axial tumors, postoperative scarring within the trigone and trauma [13],[14]. For the patient in this study, her temporal horn entrapment may be related to the decompression of the large amounts of intraventricular air distending the right ventricle creating a seal in the trigone.
Unexpectedly, the patient became shunt independent after years of VP shunt insertion and revision. One possible explanation is the temporal shunt catheter that was inserted more medially than intended for decompression of the temporal horn entrapment. The temporal shunt catheter was approaching immediately adjacent to the interpeduncular cistern on imaging. A ventriculocisternostomy may have been performed unintentionally leading to the resolution of shunt dependence. Another explanation may be the re-opening of her previous third ventriculostomy with the high intracranial pressure from shunt obstructions.
CONCLUSION
Hyperbaric oxygen treatment is an alternative treatment in neurosurgery for postoperative wound infections. Although pneumocephalus after HBOT is a very rare complication, careful evaluation of the patient is needed prior to initiating HBOT. This is the first report of pneumoventricle in the context of a non-healing VP shunt wound. Increased awareness of this potential complication of HBOT can aid in the decision-making of whether to expose patients with non-healing VP shunt incisions to this therapy.
REFERENCES
1.
Shah J. Hyperbaric oxygen therapy. J Am Col Certif Wound Spec 2010;2(1):9–13. [CrossRef]
[Pubmed]

2.
Tibbles PM, Edelsberg JS. Hyperbaric-oxygen therapy. N Engl J Med 1996;334(25):1642–8. [CrossRef]
[Pubmed]
3.
Hunt TK, Hopf HW. Wound healing and wound infection. What surgeons and anesthesiologists can do. Surg Clin North Am 1997;77(3):587–606.
[Pubmed]
4.
Larsson A, Engström M, Uusijärvi J, Kihlström L, Lind F, Mathiesen T. Hyperbaric oxygen treatment of postoperative neurosurgical infections. Neurosurg 2002;50(2):287–95.
[Pubmed]
5.
Heyboer M 3rd, Sharma D, Santiago W, McCulloch N. Hyperbaric oxygen therapy: Side effects defined and quantified. Adv Wound Care (New Rochelle) 2017;6(6):210–24. [CrossRef]
[Pubmed]
6.
Ambiru S, Furuyama N, Aono M, Otsuka H, Suzuki T, Miyazaki M. Analysis of risk factors associated with complications of hyperbaric oxygen therapy. J Crit Care 2008;23(3):295–300. [CrossRef]
[Pubmed]
7.
Lee CH, Chen WC, Wu CI, Hsia TC. Tension pneumocephalus: A rare complication after hyperbaric oxygen therapy. Am J Emerg Med 2009;27(2):257. e1–3. [CrossRef]
[Pubmed]
8.
Lee LC, Lieu FK, Chen YH, Hung TH, Chen SF. Tension pneumocephalus as a complication of hyperbaric oxygen therapy in a patient with chronic traumatic brain injury. Am J Phys Med Rehabil 2012;91(6):528–32. [CrossRef]
[Pubmed]
9.
Ugarriza LF, Cabezudo JM, Lorenzana LM, Porras LF, García-Yagüe LM. Delayed pneumocephalus in shunted patients. Report of three cases and review of the literature. Br J Neurosurg 2001;15(2):161–7. [CrossRef]
[Pubmed]
10.
Cunqueiro A, Scheinfeld MH. Causes of pneumocephalus and when to be concerned about it. Emerg Radiol 2018;25(4):331–40. [CrossRef]
[Pubmed]
11.
Spallone A, Belvisi D, Marsili L. Entrapment of the temporal horn as a cause of pure Wernicke aphasia: Case report. J Neurol Surg Rep 2015;76(1):e109–12. [CrossRef]
[Pubmed]
12.
Sharifi G, Gahdiri T, Vakilzadeh G, Nasi D. An idiopathic huge trapped temporal horn: Surgical strategy and review of literature. J Neurol Neurosci 2017;8(S4):229. [CrossRef]
13.
Bohl MA, Almefty KK, Nakaji P. Defining a standardized approach for the bedside insertion of temporal horn external ventricular drains: Procedure development and case series. Neurosurgery 2016;79(2):296–304. [CrossRef]
[Pubmed]
14.
Krähenbühl AK, Baldauf J, Gaab MR, Schroeder HWS. Endoscopic temporal ventriculocisternostomy: An option for the treatment of trapped temporal horns. J Neurosurg Pediatr 2013;11(5):568–74. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Lily Xiao Jing Sun - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Andrew Nataraj - Interpretation of data, Revising it critically for important intellectual content, Final approval of the version to be published
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Lily Xiao Jing Sun et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



