|
Case Report
Sepsis secondary to gastric reservoir after vertical gastrectomy
1 MD, General surgeon, Division of General Surgery/Laparoscopy, Centro Médico de Especialidades, Ciudad Juárez, Chihuahua, Mexico
2 MD, General surgeon, Bariatric surgeon, Division of General Surgery/Laparoscopy, Centro Médico de Especialidades, Ciudad Juárez, Chihuahua, Mexico
3 MD, General physician, Instituto de Ciencias Biomédicas, Universidad Autónoma de Ciudad Juárez, Ciudad Juárez, Chihuahua, Mexico
Address correspondence to:
Danai Hernández Carreón
Vicente Guerrero 8907, Fraccionamiento Las Quintas 32401,
Mexico
Message to Corresponding Author
Article ID: 100062S05SC2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Cereceres SJR, Jaime CAL, Avilez CTP, Carreón DH. Sepsis secondary to gastric reservoir after vertical gastrectomy. Edorium J Surg 2025;11(1):7–11.ABSTRACT
Introduction: As obesity rates have increased worldwide, bariatric surgery has become the most successful and long-lasting treatment for patients with obesity. Ever since, laparoscopic sleeve gastrectomy has gained popularity in recent years and has become the most popular bariatric procedure performed due to its effectiveness in weight loss and for being easier than other bariatric procedures.
Case Report: A 55-year-old female who underwent laparoscopic vertical gastrectomy three weeks prior to her evaluation due to epigastralgia, fever, nausea and vomiting. She was first evaluated by a surgeon, who performed surgical procedures on a weekly basis and assessed no signs of peritoneal alarm and a granuloma at the abdominal wall. Diagnostic protocol was initiated based on ultrasound, demonstrating a fistulous tract through the skin with communication to the abdominal cavity and a collection in the abdominal wall. Simple abdominal tomography was performed which demonstrated a collection in the peritoneal cavity, as well as an abscess. The patient was admitted with a diagnosis of gastric fistula plus peritoneal and abdominal wall abscess. Preoperative tests showed leukocytosis and thrombocytosis. Diagnostic laparoscopy was carried out, identifying a large plastron toward the epigastrium and a residual abscess, in addition to an apparent gastric reservoir from the gastrectomy performed.
Conclusion: Nowadays, bariatric surgery is considered extremely safe, especially since the introduction of the laparoscopic approach. This case shows a complication secondary to the high demand for bariatric procedures that lead to leaving the gastric reservoir after the gastrectomy which can lead to death.
Keywords: Gastric reservoir, Postoperative complications, Sepsis, Vertical gastrectomy
INTRODUCTION
As obesity rates have increased worldwide, bariatric surgery has become the most successful and long-lasting treatment for patients with obesity. Bariatric surgery results in long-lasting weight loss of approximately 50% to 75% of extra body weight depending on the type of surgery, in addition to the benefits of associated comorbidities. Nowadays, bariatric surgery is performed through a laparoscopic approach which has decreased postoperative complications and recovery time [1].
The sleeve gastrectomy was first introduced in 1990 and the first laparoscopic procedure was performed in 1999. Ever since, sleeve gastrectomy has gained popularity in recent years and has become the most popular bariatric procedure performed due to its effectiveness in weight loss and for being easier than other bariatric procedures, constituting 46% of all bariatric surgeries. Laparoscopic sleeve gastrectomy is a procedure in which the stomach’s capacity is reduced about 80% by resecting the greater curvature coupled with the elimination of the gastric fundus, which consequently causes a decrease in ghrelin’s concentration, promoting satiety, and limiting food intake [2],[3],[4].
Bariatric procedures are highly safe, since their laparoscopic approach, but can present early or late complications that compromise the patient’s life if not treated promptly and properly. Laparoscopic sleeve gastrectomy has a postoperative complication incidence of 2.12% and a mortality rate of 0.27%, both being lower in comparison to other bariatric procedures [2],[5].
CASE REPORT
A 55-year-old female patient with a history of high blood pressure under medical treatment with two antihypertensive drugs. The patient with a height of 1.62 meters, weight of 115 kilograms, and a body mass index of 43.8, who underwent vertical gastrectomy prior to her current re-intervention.
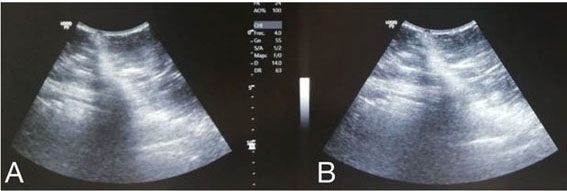
The patient presented with a history of laparoscopic vertical gastrectomy three weeks prior to her evaluation due to epigastralgia, fever of 39.5°C, asthenia, adynamia, nausea, and vomiting. She was evaluated by a surgeon, who performed surgical procedures on a weekly basis and assessed no signs of peritoneal alarm and a granuloma at the abdominal wall. The patient went to our bariatric center, where diagnostic protocol was initiated based on ultrasound, demonstrating a fistulous tract through the skin with communication to the abdominal cavity and a collection in the abdominal wall (Figure 1). Subsequently, a simple abdominal tomography was performed which demonstrated an abscessed collection in the peritoneal cavity, as well as an abscess (Figure 2). The patient was admitted with a diagnosis of gastric fistula plus peritoneal and abdominal wall abscess. Preoperative test showed a leukocytosis of 18,000 with neutrophilia, and a thrombocytosis of 600,000, the rest of clinical parameters were normal.
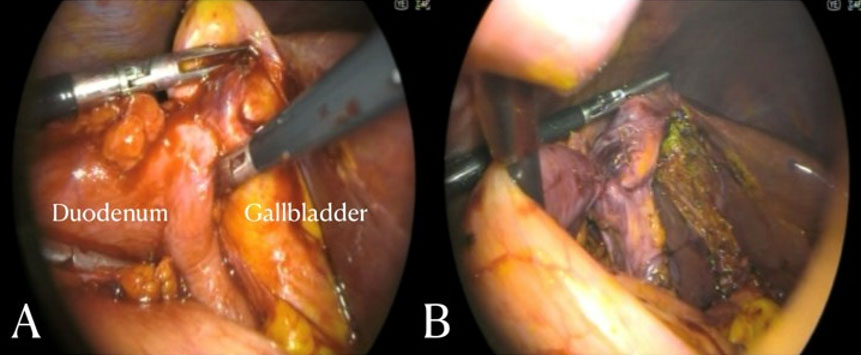
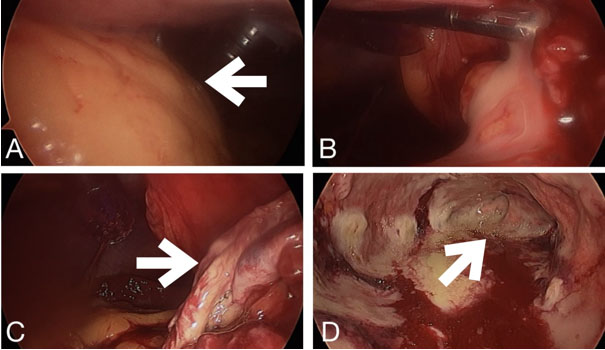
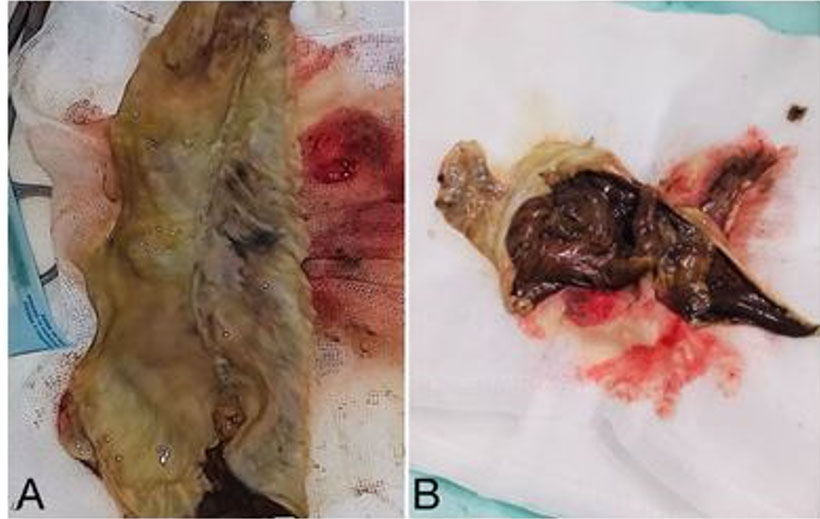
The patient was taken to the operating room, where, after general anesthesia and in a supine position, diagnostic laparoscopy was carried out. A large plastron was identified in the epigastrium and mesogastrium, which was freed and dissected (Figure 3A and Figure 3B). A residual abscess of approximately 200 cc of purulent material was found, in addition to an apparent gastric reservoir from a gastrectomy performed (Figure 3C and Figure 3D). The gastric reservoir was extracted, surgical cleansing was performed, and drains were placed (Figure 4).
In her immediate postoperative period the patient presented significant clinical improvement, no fever, tolerating oral administration, drains with serohematic output and with broad-spectrum antibiotics. The patient was discharged 72 hours after surgery with satisfactory progress.

DISCUSSION
Complications of bariatric surgery are divided into early complications, which occur within 30 days after surgery, and late complications after 30 days of the surgery. Early complications include leaks, hemorrhages, and venous thromboembolic events. Nonetheless, according to severity, complications may be classified into minor and major. Major complications include those that require early re-intervention, hemorrhages requiring transfusion, and the ones involving more than seven days of hospitalization and intensive care [5],[6].
Bleeding
Bleeding is observed in approximately 2% of all cases, constituting the most common complication after laparoscopic sleeve gastrectomy. Main risk factors are related to the patient’s comorbidities, such as high blood pressure and portal hypertension, which increases the risk of bleeding at the staple line or at the vessels of the greater curvature, and to the surgical technique. Usually, the source of hemorrhage is the staple line, an injury to the liver or spleen, and trocar site bleeding. There are several elements to reinforce the staple line such as oversewing and metallic clips. The choice of the cartridge height in relation to the thickness of the stomach is essential for bleeding prevention. Bleeding may be endoluminal manifesting as an upper gastrointestinal bleeding or intraperitoneal and most cases will resolve spontaneously. Treatment for bleeding involves revision surgery and transfusion may be necessary in some cases [2],[4],[7],[8].
Leaks
Gastric leak is the most feared complication due to the increase in morbidity and mortality. Patients with a body mass index greater than 50 and those undergoing revisional surgery are at most risk of presenting leaks. Most commonly, gastric sleeve leaks occur in the context of a high pressure system derived from the lower esophageal and pyloric sphincters. Other less common causes include stenosis or twist of the sleeve and ischemic injury in the remnant stomach. Gastric leaks may occur anywhere along the staple line; however, 85% of the cases arise from below the gastroesophageal junction. Most cases of leaks will occur within the first week, typically three days after surgery, and about 80% of those will require emergency surgery. Some leaks may be so small and can present in asymptomatic patients, while others can lead to life-threatening sepsis. Leaks may lead to abscess and fistula formation. Leak assessment should include abdominal computed tomography with oral contrast. Closing the leak either with sutures or by placing a modified Graham patch are surgical options [1],[2],[5],[9].
Portal Thrombosis
Portal thrombosis is a very rare complication after sleeve gastrectomy with an incidence of 0.3% and a mortality of 40%. It is more common after sleeve gastrectomy in comparison to other bariatric surgical interventions. Several mechanisms have been implied such as splenic ischemia, exposition, and manipulation of the splenic vein and direct trauma by retractors to the left hepatic lobe, as well as the hypercoagulable state caused by obesity. Initially patients will present nonspecific abdominal pain which will evolve to peritoneal irritation. Contrast abdominal tomography will confirm the diagnosis and the treatment will depend on the severity of the clinical presentation, some requiring bowel resection due to ischemia. Anticoagulants should be maintained for up to six months [3],[4],[7].
Stenosis
The incidence of gastric stenosis after laparoscopic sleeve gastrectomy is 1%, which increases to 10% in revision surgeries. Two types of stenosis have been described. Anatomical stenosis is caused by a wrong placement of the calibration bougie or by a running suture on the staple line and is usually located at the incisura angularis. While functional stenosis is caused by localized twist or by a spiral course of gastric stapling. Patients present with food intolerance, dysphagia, salivation, nausea, and vomiting. Upper gastrointestinal contrast study may show narrowing of the sleeve; however, upper endoscopy is diagnostic and therapeutic. Endoscopic pneumatic dilation is considered the first treatment choice for stenosis, commonly requiring from 2 to 3 dilations before achieving the desired gastric diameter [2],[3],[6],[7].
Infections
Infections are a risk for any surgical procedure. Patients undergoing bariatric surgery have a higher risk of developing infections due to associated comorbidities. The most common form of presentation is surgical site infection [1].
CONCLUSION
Nowadays, bariatric surgery is considered extremely safe, especially since the introduction of the laparoscopic approach and, therefore, morbidity rates have decreased due to advances in technology. In recent years, vertical gastrectomy has become so popular that unfortunately in many places in the world it is not performed by bariatric surgeons. There are fundamental steps that have demonstrated greater safety for bariatric patients. The percentage of this complication is extraordinarily low because it is most likely a very important error that it is not reported. Reason why surgeons should be very precise at observing micro- and macroscopic details during highly specialized training. This case shows an uncommon complication, of which no literature was found on a similar case, secondary to the high demand for bariatric procedures that lead to leaving the gastric reservoir after the vertical gastrectomy, a catastrophic error that can lead to sepsis and consequently death.
REFERENCES
1.
Tsenteradze T, Fayyaz F, Ekhator C, et al. Navigating bariatric surgery: Understanding and managing short-term and long-term complications. Cureus 2023;15(11):e48580. [CrossRef]
[Pubmed]

2.
Wo?niewska P, Diemieszczyk I, Hady HR. Complications associated with laparoscopic sleeve gastrectomy – A review. Prz Gastroenterol 2021;16(1):5–9. [CrossRef]
[Pubmed]
3.
Park JY. Diagnosis and management of postoperative complications after sleeve gastrectomy. J Metab Bariatr Surg 2022;11(1):1–12. [CrossRef]
[Pubmed]
4.
Climaco K, Ahnfeldt E. Laparoscopic vertical sleeve gastrectomy. Surg Clin North Am 2021;101(2):177–88. [CrossRef]
[Pubmed]
5.
Lim R, Beekley A, Johnson DC, Davis KA. Early and late complications of bariatric operation. Trauma Surg Acute Care Open 2018;3(1):e000219. [CrossRef]
[Pubmed]
6.
Zerrweck C, Vargas-Sahagúno CM. Complicaciones en cirugía bariátrica. Revista de la Sociedad Peruana de Cirugía Endoscópica 2023;4(1).
7.
Iannelli A, Treacy P, Sebastianelli L, Schiavo L, Martini F. Perioperative complications of sleeve gastrectomy: Review of the literature. J Minim Access Surg 2019;15(1):1–7. [CrossRef]
[Pubmed]
8.
Kassir R, Debs T, Blanc P, et al. Complications of bariatric surgery: Presentation and emergency management. Int J Surg 2016;27:77–81. [CrossRef]
[Pubmed]
9.
Raspante LBP, Barquette ÁDC, Motta EGPC, Ribeiro MA, Ramos LFM, Moreira W. Review and pictorial essay on complications of bariatric surgery. Rev Assoc Med Bras (1992) 2020;66(9):1289–95. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
We thank the staff of Centro Medico de Especialidades for their support and constant drive to learn.
Author ContributionsSaul Jasam Ruiz Cereceres - Substantial contributions to conception and design, Analysis of data, Revising it critically for important intellectual content, Final approval of the version to be published
Cesar Alberto López Jaime - Substantial contributions to conception and design, Analysis of data, Revising it critically for important intellectual content, Final approval of the version to be published
Carlos Tadeo Perzabal Avilez - Substantial contributions to conception and design, Analysis of data, Interpretation of data, Revising it critically for important intellectual content, Final approval of the version to be published
Danai Hernández Carreón - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Saul Jasam Ruiz Cereceres et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.