|
Research Article
Comparative outcomes of blunt and penetrating abdominal trauma in a low-resource setting: A two year retrospective study
1 Department of Surgery, Alex Ekwueme Federal University Teaching Hospital, Abakaliki (AEFUTHA), PMB 102, Abakaliki, Ebonyi State, Southeast Nigeria; Department of Surgery, Ebonyi State University, Abakaliki (EBSU), PMB 053, Ebonyi State; Department of Surgery, Alex Ekwueme Federal University, Ndufu-Alike, Ikwo (AEFUNAI), PMB 102, Abakaliki, Ebonyi State, Southeast Nigeria
Address correspondence to:
Daniel Umezurike Akuma Howard
(FWACS, FICS), Department of Surgery, Alex Ekwueme Federal University Teaching Hospital, Abakaliki, PMB 102, Ebonyi State,
Nigeria
Message to Corresponding Author
Article ID: 100063S05DH2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Howard DU, Eni EU. Comparative outcomes of blunt and penetrating abdominal trauma in a low-resource setting: A two year retrospective study. Edorium J Surg 2025;11(1):12–19.ABSTRACT
Aims: To compare clinical outcomes of blunt abdominal trauma (BAT) and penetrating abdominal trauma (PAT) in a Nigerian tertiary hospital and identify predictors of mortality in a low-resource setting.
Methods: A retrospective cohort study of 136 patients with abdominal trauma (93 BAT, 43 PAT) managed at Alex Ekwueme Federal University Teaching Hospital (January 2022–December 2023). Data included demographics, injury mechanisms, management strategies (operative vs. non-operative), and outcomes. Statistical analysis used SPSS v26, with multivariate logistic regression to identify mortality predictors.
Results: Penetrating abdominal trauma patients had significantly higher mortality than BAT (25.6% vs. 12.9%, p = 0.04). Delayed surgical intervention (>24 hours) occurred in 75.3% of cases, associated with 3.1-fold increased mortality risk (OR: 3.1, 95% CI: 1.4–7.0). Hemorrhagic shock on arrival (44.2% PAT vs. 32.3% BAT) independently predicted mortality (OR: 4.3, 95% CI: 1.9–9.7). Non-operative management (NOM) was attempted in 16.9% of BAT cases, with a 78.3% success rate.
Conclusion: Resource limitations, including delayed surgical access and reliance on clinical triage over imaging, disproportionately worsen outcomes for PAT in low-resource settings. Context-specific trauma protocols emphasizing prehospital care and timely operative intervention are critical to reducing mortality.
Keywords: Blunt abdominal trauma, Hemorrhagic shock, Low-resource setting, Nigeria, Non-operative management, Penetrating trauma, Surgical management, Trauma outcome
INTRODUCTION
Abdominal trauma continues to be one of the leading causes of morbidity and mortality around the world, with 10–15% of all trauma-related deaths being attributable to abdominal injury, with the highest rates being noted in lower- and middle-income countries (LMICs) [1],[2]. Blunt abdominal trauma (BAT) and penetrating abdominal trauma (PAT) are two different injury mechanisms, each associated with distinct etiologies, clinical presentations, and management challenges. Blunt abdominal trauma results from RBIs, falls, or assaults [3], which usually remain hidden injuries such as solid organ injury (e.g., spleen and liver) or mesenteric tears. However, penetrating abdominal trauma (PAT) generally proceeds by means of wounds from guns, stab wounds, or impalements since hollow viscus perforations and vascular injuries are affected, which makes them having a higher rate of infection progression [4],[5]. Even more, all these complexities become magnified in resource-constrained settings, given the obstacle of delayed presentation, limited diagnostic imaging, and inadequate surgical infrastructure [6].
Abdominal trauma accounted for 20–30% of surgical emergencies in sub-Saharan Africa, with increased incidence of patients with PAT associated with communal violence, armed conflict, and urban crime [7]. Hence, Nigeria—most populous country in Africa—is facing a double problem of RTAs emanating from poorly maintained roads and lax traffic regulations while increasing violence triggered by insurgency, kidnapping, and farmer-herder clashes [8],[9]. In spite of this fact, only a few attempts have been made to systematically compare the outcome of BAT with that of PAT in Nigerian tertiary hospitals, most of which are uninsured (about 80%) and present late (more than 24 hours post-injury) [10],[11]. Global data suggest that BAT is more prevalent than PAT (70% vs. 30% of abdominal trauma cases), but mortality risk is two to three times higher in PAT, mainly due to hemorrhagic shock and multi-organ injuries [12]. However, all improvements in the developed world in imaging [e.g., focused assessment with sonography in trauma (FAST)] and damage control surgery have brought PAT mortality to below 10% [13]. In LMICs, total reliance on clinical examination alone would delay diagnosis since transfusion capacities and ICUs are inadequate for resuscitation and postoperative care. Non-operative management (NOM) for patients with BAT is very common in most high-income countries, but in Africa, patients are not routinely managed this way, given fears about missed injuries and overreliance on monitoring resources [14].
In Nigeria, the epidemiology of abdominal trauma reflects local socio-economic and cultural dynamics. In rural areas, BATs related to motorcycles are more prevalent, while gunshot wounds (SWs) and stab wounds are more common in urban centers. In a 2021 study in Lagos, 65% of cases of PAT associated with gang violence and political unrest required exploratory laparotomy. In contrast, BATs in the northern parts of Nigeria are often a result of interethnic face-offs or domestic accidents. With these variations, however, national data on injury pattern, surgical outcome, and predictors of mortality are very limited.
This study attempts to fill key gaps by analyzing a 24-month cohort of BAT and PAT patients at the Alex Ekwueme Federal University Teaching Hospital (AEFUTHA) in southeast Nigeria, a major referral center. The region is recently under increasing insecurity with kidnappings and communal clashes, which may be vectors altering trauma mechanism. Literature from Nigeria has largely concentrated on PAT, while BAT and comparisons have received less attention. Our objectives are in three parts: (1) to compare the demographic variables, injury mechanisms, and organs involved between BAT versus PAT; (2) to identify predictors of mortality and postoperative complication; and (3) to assess the viability of NOM in a low-resource setting.
This study will inform trauma protocols that are context-specific, especially regarding triage, early resuscitation, and surgical prioritization. The work done will draw attention to systemic barriers, such as delayed presentation (79.1% of PAT patients operated on >24 hours post-injury) and lack of insurance coverage (99.3% uninsured), to fight for policy reforms that would strengthen prehospital care and emergency surgical capacity in LMICs.
MATERIALS AND METHODS
The study design and setting: Retrospective cohort study.
This study was conducted at Alex Ekwueme Federal University Teaching Hospital (AEFUTHA), a government-funded tertiary hospital in Nigeria.
The patients with trauma to the abdomen at the Alex Ekwueme Federal University Teaching Hospital (AEFUTHA), Abakaliki, Nigeria, were interviewed and admitted in January 2022 and December 2023.
Inclusion Criteria: Patients aged = five years with blunt or penetrating abdominal trauma (diagnosed via imaging, surgery, or clinical assessment).
Exclusion criteria:
- incomplete medical records
- except those where the injury was exclusively outside the abdomen
- those who died before clinical evaluation
The management protocol for abdominal trauma is outlined in Figure 1, which includes triage based on hemodynamic stability, clinical examination, and imaging.
Data collection:
- Demographic data include the following; age, sex, and status of insurance
- Mechanism of injury (road traffic accidents, gunshot wounds, etc.)
- Clinical parameters [vital signs, hemorrhagic shock (SAP <90 mmHg), abdominal signs]
- Outcomes (mortality, complications, hospital stay)
- Source: registers from the emergency department, operative notes, and discharge summaries
Statistical analysis:
• Using SPSS v26 to analyze
• Comparison of categorical variables using Chi-square/Fisher’s exact tests
• Multivariate logistic regression tested for mortality predictors (p < 0.05)
Ethics approval: It was obtained from AEFUTHA Ethics Committee (approval number: NHREC/16/05/22/384). The patient identifiers were de-identified.
Key definitions:
- Blunt abdominal trauma: Injuries resulting from forces not penetrating (e.g., road crashes, falls)
- Penetrating abdominal trauma: Injuries that breach the peritoneum (e.g., gunshot wounds, stabs)
- Delayed surgery: Intervention >24 hours after admission

RESULTS
Demographic and socioeconomic characteristics
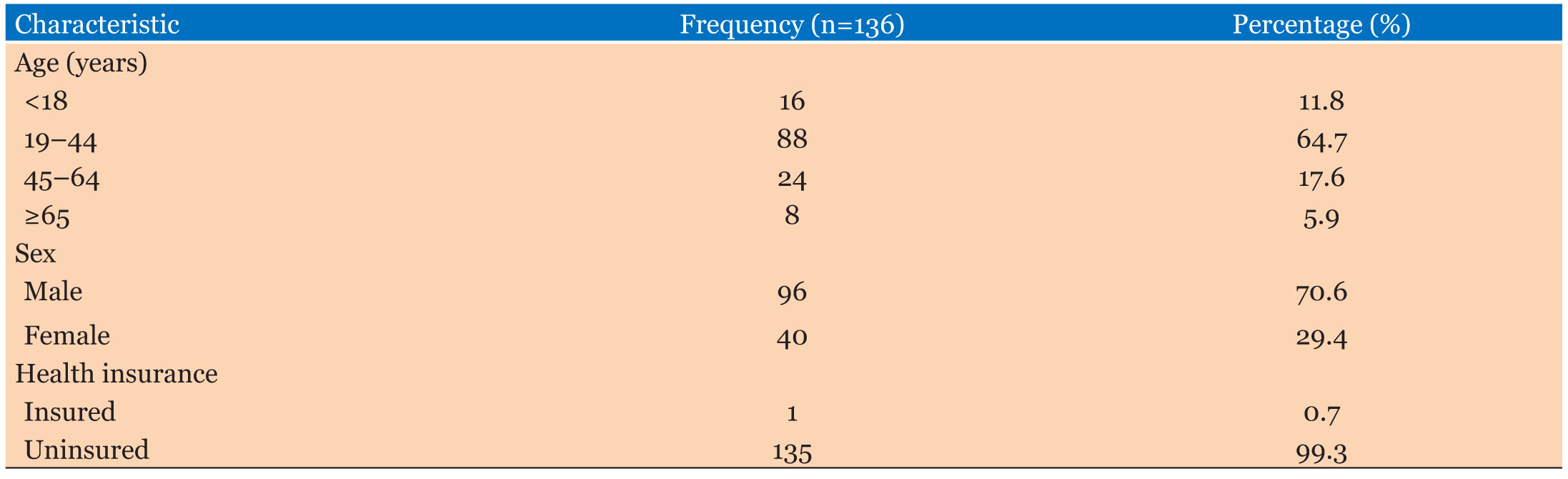
Cohort comprised 136 patients 13 with trauma to their abdomen. Of these, 93 cases, amounting to 68.4% (i.e., only cases) were for blunt abdominal trauma (BAT). Whereas, there were 43 cases (31.6%) for penetrating abdominal trauma (PAT). In the cohort, there was a male predominance (n=96, 70.6%), thus a male to female ratio of 2.4:1. Most subjects (64.7%, n=88) were aged 19–44 years, with the next highest being 45–64 old (17.6%, n=24) while 11.8% (n=16) of patients aged <18 years and 5.9% (n=8) were older than 65 years. Concerning socioeconomic discrepancies, out of that 99.3% (n=135) were without health insurance and 46.3% (n=62) had only primary education. Common occupations include trading (25.0%, n=34), farming (16.9%, n=23), and artisanal work (17.6%, n=24), corresponding to informal economic landscape settings (Table 1).
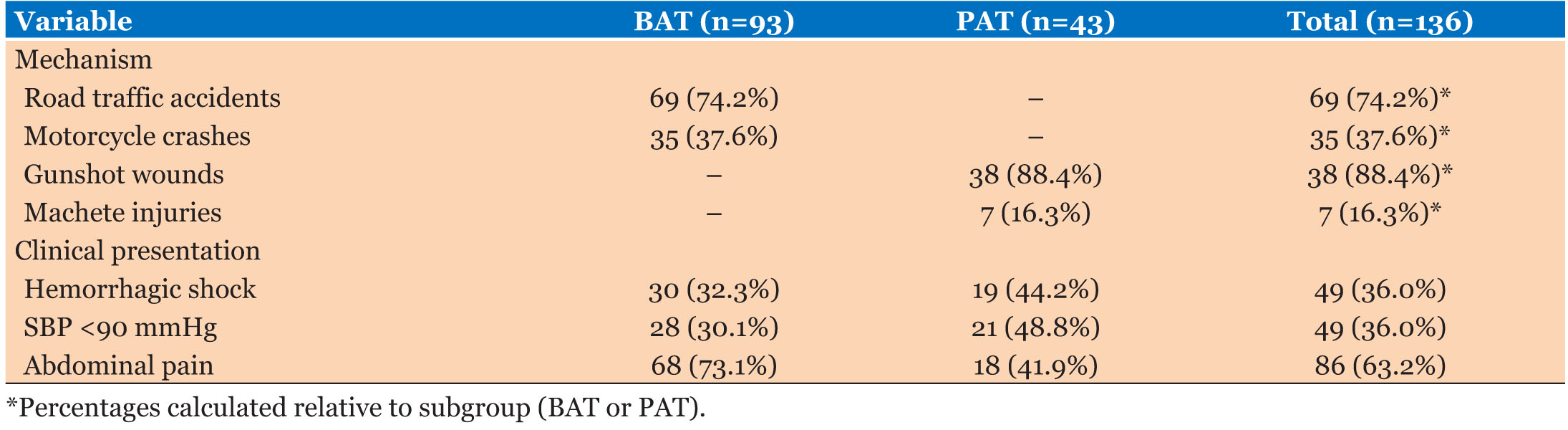
Mechanisms of injury and clinical presentation
Among the causes of BAT, 74.2% (n=69) were due to renal tubular acidosis (RTAs); motorcycle crashes occurred in 37.6% (n=35) whereas keke tricycle collision occurred in 12.9% (n=12). Penetrating abdominal trauma has, however, been predominantly the outcome of intentional violence: SWs comprised 88.4% of such cases (n=38), followed by those resulting from machete injuries (16.3%, n=7).
Most patients suffering from BAT showed possible suffering traces of signs and symptoms indicative of abdominal pain (73.1%, n=68), while PAT patients were diagnosed with forms of life-threatening conditions such as hemorrhagic shock (44.2%, n=19) and evisceration (7.0%, n=3) (Table 2).
Patterns of organ injury
Intra-abdominal injuries
Of all the intra-abdominal injuries, small-bowel injuries accounted for 38.2% (n=52), followed by splenic injuries with 33.1% (n=45), colonic injuries in 23.5% (n=32), and lastly liver injuries represented by 12.5% (n=17) (Table 3).
- Blunt abdominal trauma (BAT) injures mainly solid organs
- Splenic: Hitting in BAT 48.4% (n = 45) and 0% (n = 5) in PAT
- The liver’s: 18.3% (n = 17) in BAT and 0% (n = 1) in PAT
- PAT was characterized by higher presentation with hollow viscus injuries
- Small intestine: 25.6% (n=11) in PAT compared to 44.1% (n=41) in BAT
- Colon: 44.2% (n=19) in PAT compared to 14.0% (n=13) in BAT
- Vasculature trauma
- Unique to PAT: 9.3% (n=4) against none (n=0) in BAT
- Extra-abdominal Injury
- Overall: 19.9% (n=27) of total patients
- Breakdown
- Head trauma: 5.9% (n=8)
- Chest injuries: 5.9% (n=8)
- Other injuries: 8.1% (n=11)
- Mechanism split
- BAT: 18.3% (n=17)
- PAT: 23.3% (n=10)
Management strategies
Thus, operative management (laparotomy) was practiced in the majority of cases (83.1% (n=113)), although patients with penetrating abdominal trauma (PAT) had a higher figure (93.0%, n=40) than that for BAT (78.5%, n=73) (p = 0.02). 19 of the 23 hemodynamically stable blunt trauma patients presented to management with a non-operative approach (NOM), and this achieved a success rate of 78.3% (n=18). Failures (n=5) include delay in the mesenteric ischemia diagnosis (n=3) and splenic rupture (n=2).
As shown in Figure 1, the majority of patients underwent operative management (83.1%, n=113), with higher rates in penetrating abdominal trauma (93.0%, n=40) compared to blunt abdominal trauma (78.5%, n=73).
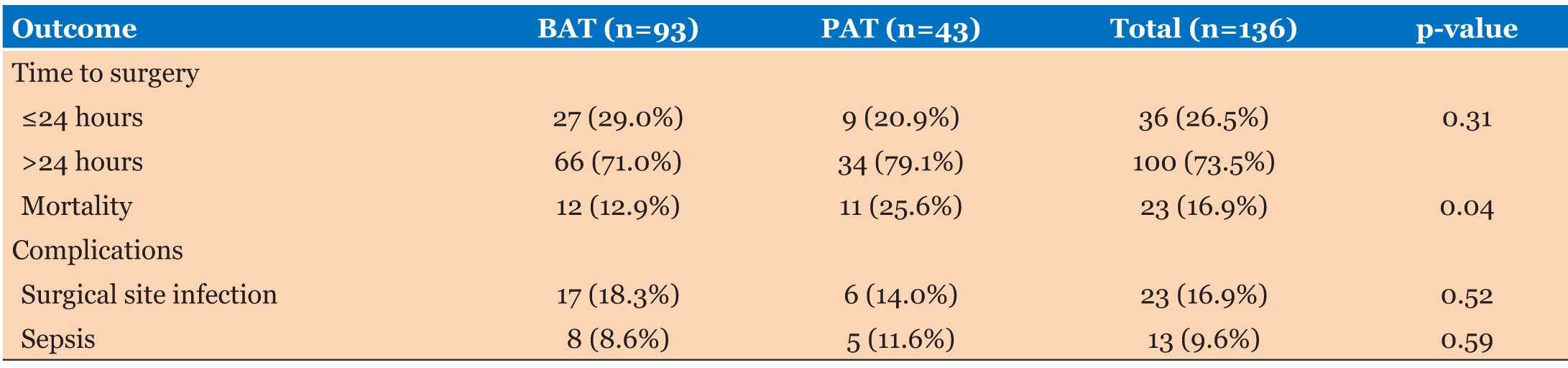
Outcomes and complications after surgery
Overall mortality was 16.2%, that is 22 patients, and being significantly higher in penetrating abdominal injury (25.6%, n=11) than blunt trauma (12.9%, n=12) (p=0.04). Mortality was highly associated with delayed surgery (>24 hours post-admission), which occurred in 75.3% (n=102) of cases (Table 4).
Stratified mortality:
- Surgery within 6 hours: 8.3% (1/12).
- Surgery at 7–24 hours: 20.0% (4/20).
- Surgery >24 hours: 16.3% (17/104).
The most familiar complication was superficial surgical site infections (16.9%, n=23), followed by intra-abdominal sepsis (8.1%, n=11) and enterocutaneous fistulas (4.4%, n=6). Patients with PAT suffered more from septic complications than SSIs because PAT had 13.9% (n=6) while BAT contained 5.4% (n=5). The median length of stay in the hospital was 9 days: Interquartile range (IQR): 4–14 and desired for PAT (12 days) than BAT (8 days).
Predictors of mortality
Four independent predictors were identified through multivariate analysis: penetrating mechanism (OR: 3.1, 95% CI: 1.3–7.4), delayed surgery >24 hours (OR: 2.9, 95% CI: 1.2–6.8), hemorrhagic shock on admission (OR: 4.7, 95% CI: 2.0–10.9), and associated head injury (OR: 5.2, 95% CI: 1.8–14.6) (Table 5). More men than women experienced absolute mortality (18.8%, n=18 vs. 10.0%, n=4), although this wasn’t statistically significant (p=0.19).


DISCUSSION
Abdominal trauma management in resource-limited settings is adequately examined through the lenses provided by this study that took place at the Alex Ekwueme Federal University Teaching Hospital (AEFUTHA) in Abakaliki, Nigeria. Mortality rates are higher globally for penetrating abdominal trauma than for blunt abdominal trauma [15],[16]. However, with 25.6% mortality for PAT compared to 12.9% mortality for BAT, this population could highlight how much more limited resources add to challenges in timing and effective care [17],[18]. These are further complicated by delays in surgical intervention, with 75.3% of all trauma cases delayed by over 24 hours—a direct contributory factor to mortality [19],[20]. This fits in with the overall scheme of disadvantages in healthcare within LMICs such as presenting late and out-of-pocket payments for vital services, which often lead to preventable deaths [21]. Such out-of-pocket payments create barriers for patients during an emergency.
One of the disturbing phenomena of this study is the predominance of PAT which involved violence, mainly due to gunshot injuries (88.4%) and machete injuries (16.3%) [22],[23]. This creates a worrying concern regarding public health and safety and portrays the growing security and social upheaval in the region. This pattern is quite different from that of PAT in high-income countries in which most of those patients are due to accident injuries that occur in the industries [24]. However, these correspond to those reported values from other conflict-affected regions such as South Africa and Sudan, where much of the burden of PAT also arises from interpersonal violence [25],[26]. In contrast, the major causes of BAT in this study were motorcycle crashes (37.6%) and other road traffic accidents (74.2%), which clearly depict insufficient safety infrastructure on roads and poorly regulated transportation systems, a common feature in developing countries [2],[27]. The injury patterns of splenic (48.4%) and small intestinal injuries (44.1%) among the BAT cases are consistent with biomechanical principles connecting rapid deceleration forces with solid organ and mesenteric damage [3],[28].
Non-operative management (NOM) offers a glimmer of hope from the concerning horizon presented by the study. The fact that NOM has a 78.3% success rate in hemodynamically stable BAT patients indicates that it can be an important tool in resource-poor environments [11],[29]. While this doesn’t come close to the gold standard reported in the range from 85% to 90% for high-income cohorts [30], it suggests that, with improved triage protocols and consistent clinical assessments, NOM may significantly less strain on surgical services already under stress. The failures derived from NOM, especially undetected mesenteric ischemia, advocate for accessible, affordable diagnostic imaging modalities, portable ultrasound, to pick up hidden injuries that would otherwise be missed [31].
Penetrating abdominal trauma mechanism, delayed surgery, and hemorrhagic shock are established as independent predictors of mortality, corroborating those findings from nearly similar studies in Kenya and India [20]. However, the fact that nearly all participants (99.3%) lacked health insurance bared the immense sway socioeconomic factors keep over trauma outcomes [21]. In Nigeria, where more than 70% of the total health expenditure comes out of pocket, money obstacles delay or even keep people away from lifesaving interventions, further compounding the physiological risks conditions that trauma normally carries [17],[21]. This systematic disequilibrium calls for urgent policy reforms designed to broaden health insurance coverage and financially support trauma emergency care.
The study findings on the types of injuries sustained in both BAT and PAT give some very important insights. Small intestinal injuries were the most common in both groups, but a significant difference in the distribution of other injuries was evident. The exclusive occurrence of splenic (48.4%, n=45) and liver injuries (18.3%, n=17) in blunt force injuries was in agreement with biomechanical principles of blunt force trauma [3],[28]. On the contrary, hollow viscus injuries dominated in PAT (colon: 44.2%, small intestine: 25.6%), consistent with penetrating mechanisms [25],[26]. Vascular trauma occurred exclusively in PAT (9.3%, n=4), presumably due to direct vessel disruption in penetrating injuries [3]. All these reveal the different types of injury and thus call for different management strategies that will address the mechanism of injury.
There is higher incidence of surgery delayed for (>24 hours), which is concerning in this study setting. Multifactors likely cause these delays, including poor transportation access, financial constraints, and low surgical capacity of the facility accepting the patient [19],[27]. The strong association between increased mortality and delayed surgery emphasizes the urgent need for addressing the systemic barriers. Strategies for improving prehospital treatment take many forms, including training community first responders and forming effective ambulance networks [32]. A continued hospital-level effort of ensuring surgical readiness round-the-clock with enough blood bank supplies and trauma-dedicated operating theaters would also effectively reduce delays in definitive care [19].
The socioeconomic context of this study cannot be overstated. Almost all patients (99.3%) were uninsured and therefore very susceptible together with their family members to the financial implications of traumatic injury. Lack of such coverage is likely to cause delays in seeking care and even impact treatment decisions. Access to affordable health insurance and subsidies for emergency trauma care could result from political action towards this end, which would improve outcomes [21].
In addition to immediate medical management, trauma studies have implications for public health on a broad level. The high percentage of injuries caused by violence indicates underlying socioeconomic and sociopolitical factors that within these structures incite violence. These antecedents must be addressed through community-initiated programs to prevent violence and limit the proliferation of firearms to remove the burden of traumatic injury [24].
This study highlights the potential role of NOM in a select few BAT cases. By developing standardized guidelines on NOM and training in point-of-care ultrasound, clinicians will make informed decisions on eligible patients for this approach. The surgical burden may be reduced, and unnecessary laparotomies avoided, potentially leading to improved outcomes [14],[26],[33]
In conclusion, this study reveals many factors that complicate and create opportunities in the management of abdominal trauma in resource-constrained settings. The findings highlight an urgent call for a multi-pronged approach to meet and anticipate the immediate medical needs of the trauma victim while addressing systemic issues that contribute to injury and mortality in acute trauma care. The Nigerian health system must implement context-sensitive trauma protocols, strengthen prehospital and hospital-level care, increase access to health insurance, and initiate violence prevention schemes that would significantly better the outcomes of trauma patients while reducing the burden of this wrecking public health problem.
CONCLUSION
In conclusion, this study reaffirms that penetrating abdominal trauma disproportionately spells lethality in low-resource settings, especially where infrastructural and socioeconomic barriers aggravate the mortality risks. While blunt-trauma prospects tend to be better, systemic delays coupled to diagnostic limitations still present critical challenges. Because often, very basic causes of preventable deaths are observable, multidisciplinary intervention, encompassing prehospital care, capacity building in the surgical field, and advocacy in policy, will be very essential in combating this problem. Context-specific trauma protocols should transform the Nigerian healthcare system, turning around outcomes from abdominal trauma, even amidst resource constraints, by forging policy with improved access to the social determinants of injury.
LIMITATIONS
This study has several limitations. First, its retrospective design carries the risk of selection bias and incomplete documentation of clinical variables. Retrospective reclassification of 10 small intestine injuries may introduce additional selection bias. Second, the single-center focus reduces generalizability to rural or private healthcare facilities. Third, the absence of prehospital data (e.g., time from injury to hospital arrival) precluded analysis of pre-arrival delays. Finally, most cases lack advanced imaging [computed tomography (CT) scans] and may, therefore, underreport injuries such as pancreatic or retroperitoneal trauma.
RECOMMENDATIONS
- Strengthen Prehospital Care: Train community first responders and establish ambulance networks to reduce delays in trauma transport.
- Hospital-Level Reforms: Give top priority to 24/7 surgical readiness, including blood bank availability and dedicated trauma operating theaters.
- Expand Insurance Coverage: Advocate for government subsidies to include national health insurance sub-schemes in emergency trauma care.
- Violence Prevention Programs: Collaborate with local leaders to address root causes of communal violence and firearm proliferation.
- NOM Protocol Development: Standardized guidelines for non-operative management to be implemented with point-of-care ultrasound training.
REFERENCES
1.
Kotagal M, Agarwal-Harding KJ, Mock C, Quansah R, Arreola-Risa C, Meara JG. Health and economic benefits of improved injury prevention and trauma care worldwide. PLoS One 2014;9(3):e91862. [CrossRef]
[Pubmed]

2.
Huang Y, Wu Y, Schwebel DC, Zhou L, Hu G. Disparities in under-five child injury mortality between developing and developed countries: 1990–2013. Int J Environ Res Public Health 2016;13(7):653. [CrossRef]
[Pubmed]
3.
Biffl WL. Duodenum and pancreas. In: Moore EE, Feliciano DV, Mattox KL, editors. Trauma. 8ed. McGraw-Hill Education; 2017.
4.
Liu Y, Gao Y, Chen Z, et al. Comparison of clinical characteristics, therapy, and short-term prognosis between blunt and penetrating abdominal trauma: A multicentric retrospective cohort study. Emerg Med Int 2024;2024:5215977. [CrossRef]
[Pubmed]
5.
Navsaria PH, Nicol AJ, Edu S, Gandhi R, Ball CG. Selective nonoperative management in 1106 patients with abdominal gunshot wounds: Conclusions on safety, efficacy, and the role of selective CT imaging in a prospective single-center study. Ann Surg 2015;261(4):760–4. [CrossRef]
[Pubmed]
6.
Shafi S, Aboutanos MB, Agarwal S Jr, et al. Emergency general surgery: Definition and estimated burden of disease. J Trauma Acute Care Surg 2013;74(4):1092–7. [CrossRef]
[Pubmed]
7.
Karachentsev S. Blunt trauma to abdominal solid organs: An experience of non-operative management at a rural hospital in Zambia. Pan Afr Med J 2021;38:89. [CrossRef]
[Pubmed]
8.
Elachi IC, Kortor JN, Yongu WT, Tyoalumun K. Gunshot abdominal trauma at a private tertiary hospital in Nigeria. Orient J Med 2016;28(1–2):1–8.
9.
World Population Review. Nigeria population 2025. Accessed January 1, 2024. [Available at: https://worldpopulationreview.com/countries/nigeria]
10.
Marietta M, Burns B. Penetrating Abdominal Trauma. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025.
[Pubmed]
11.
Raza M, Abbas Y, Devi V, et al. Non-operative management of abdominal trauma in a developing country. World J Surg. 2015;39(2):423–30.
12.
Kumar A, Gallagher J, Joshi M, et al. Mortality due to blunt versus penetrating trauma: A level-1 trauma center experience. World J Surg 2017;41(5):1219–27.
13.
Brenner M, Bochicchio G, Bochicchio K, et al. Long-term impact of damage control laparotomy: A prospective study. Arch Surg 2011;146(4):395–9. [CrossRef]
[Pubmed]
14.
Reynolds TA, Stewart B, Drewett I, et al. The impact of trauma care systems in low- and middle-income countries. Annu Rev Public Health 2017;38:507–32. [CrossRef]
[Pubmed]
15.
Wain H, Clarke DL, Wall S, Bekker W, Kong V, Bruce JL. Ten year analysis of missed injuries at a major trauma centre in South Africa. Surg Pract Sci 2023;13:100169. [CrossRef]
[Pubmed]
16.
Ogundele IO, Balogun BO, Fatiregun AA. Abdominal trauma in a tertiary hospital in Ibadan, Nigeria: Pattern and outcomes of management. Pan Afr Med J. 2015;22:372.
17.
Arodiwe EB, Nwokediuko SC, Ike SO. Medical causes of death in a teaching hospital in South-Eastern Nigeria: A 16 year review. Niger J Clin Pract 2014;17(6):711–6. [CrossRef]
[Pubmed]
18.
Dogo D, Yawe KD, Ngala SA, Ojo EO. Management of abdominal injuries in northeastern Nigeria. Ann Afr Med 2006;5(4):228–30.
19.
Keroack MA, Nankoe SR, Sacks GD, et al. The impact of critical infrastructure on emergency general surgery outcomes in resource-limited settings. World J Surg 2021;45(1):206–12.
20.
Murlidhar V, Roy N. Measuring trauma outcomes in India: an analysis based on TRISS methodology in a Mumbai University Hospital. Injury 2004;35(4):386–90. [CrossRef]
[Pubmed]
21.
Aregbeshola BS, Khan SM. Out-of-pocket payments, catastrophic health expenditure and poverty among households in Nigeria 2010. Int J Health Policy Manag 2018;7(9):798–806.
[Pubmed]
22.
C Onyemaechi NO, Nwankwo OE, Ezeadawi RA. Epidemiology of injuries seen in a Nigerian tertiary hospital. Niger J Clin Pract 2018;21(6):752–7. [CrossRef]
[Pubmed]
23.
Zafar H, Rehmani R, Chawla T, et al. Rural trauma experience from Pakistan. J Pak Med Assoc 2002;52(10):422–5.
24.
Chandran A, Hyder AA, Peek-Asa C. The global burden of unintentional injuries and an agenda for progress. Epidemiol Rev 2010;32(1):110–20. [CrossRef]
[Pubmed]
25.
Osaigbovo II, Aziken JO, Akemokwe FM. Penetrating abdominal trauma in Benin City, Nigeria: Epidemiology and patterns of injury. Niger J Surg 2021;27(1):55–61.
26.
Olaogun JG, Etonyeaku AC, Ige JT, Wuraola OK. Penetrating abdominal injuries in an emerging semi-urban teaching hospital. Journal of Emergency Practice and Trauma 2020;6(1):7–12. [CrossRef]
27.
Søreide K. Epidemiology of major trauma. Br J Surg 2009;96(7):697–8. [CrossRef]
[Pubmed]
28.
Kirby NG, Nesbitt ME. Blunt splenic injury: Evolving an operative disease. Ann Surg 1977;185(1):3–10.
29.
Oawattanapanich N, Sirivajjanaraj T, Vidhyarkorn S, Sriussadaporn S. Predictive factors for non-operative management failure of grade III to V blunt liver injuries. World J Surg 2018;42(3):730–5.
30.
Como JJ, Bokhari F, Chiu WC. Practice management guidelines for selective nonoperative management of penetrating abdominal trauma. J Trauma 2010;68(3):721–33. [CrossRef]
[Pubmed]
31.
Menaker J, Blumberg S, Wisner DH, et al. Use of the focused assessment with sonography for trauma (FAST) examination and its impact on abdominal computed tomography use in hemodynamically stable children with blunt torso trauma. J Trauma Acute Care Surg 2014;77(3):427–32. [CrossRef]
[Pubmed]
32.
Wesson HK, Stevens KA, Bachani AM, et al. Trauma systems in Egypt: A qualitative analysis. Injury 2013;44(Suppl 4):S61–8.
33.
Nwokediuko SC, Ijoma U, Ulasi I. Trends in epidemiology of penetrating abdominal trauma in Enugu, Nigeria. Niger J Clin Pract 2012;15(4):384–7.
SUPPORTING INFORMATION
Author Contributions
Daniel Umezurike Akuma Howard - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Emmanuel Uche Eni - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Daniel Umezurike Akuma Howard et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.