|
Case Series
Rib fixation: New horizons in regional surgery
1 General Surgery Unit, Goulburn Valley Health, 2/2-48 Graham Street, Shepparton VIC 3630, Australia
2 General Surgery Unit, Mackay Hospital and Health Service, 475 Bridge Road, Mackay QLD 4740, Australia
3 Upper Gastrointestinal and Hepatopancreaticobiliary Unit, Cairns and Hinterland Hospital and Health Service, 165 The Esplanade, Cairns, QLD 4870, Australia
Address correspondence to:
Xin Yi Goai
2/2-48 Graham Street, Shepparton, VIC 3630,
Australia
Message to Corresponding Author
Article ID: 100064S05II2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Indigahawela I, Shi W, Goai XY, Dlaska C, Dissanayake M, Pretorius C, Beardsley C. Rib fixation: New horizons in regional surgery. Edorium J Surg 2025;11(2):1–9.ABSTRACT
Introduction: Rib fractures are a common consequence of trauma, often necessitating surgical stabilization for improved outcomes. Mackay Base Hospital (MBH) serves as a regional center for managing trauma cases, including rib fractures. Despite logistical challenges, MBH strives to provide optimal care for patients requiring surgical stabilization of rib fracture (SSRF). This article aims to provide insight into SSRF practices at MBH.
Case Series: A retrospective analysis of patients undergoing SSRF at MBH from January 2021 to June 2022 was conducted. Five SSRF procedures were performed, with a mean patient age of 56 years and a predominance of male patients. Postoperatively, extubation occurred within 48 hours in most cases. One morbidity and one mortality were reported, both unrelated to surgical complications.
Conclusion: Despite logistical and resource-related challenges, MBH demonstrated successful implementation of SSRF. Structured upskilling, multidisciplinary coordination, and investment in local capabilities suggest that regional centers can deliver safe and effective SSRF care.
Keywords: Chest trauma, Regional surgery, Rib fractures, Surgical stabilization of rib fractures, Thoracic surgery
INTRODUCTION
Chest trauma is associated with significant mortality and morbidity, with rib fractures identified in approximately two-thirds of cases [1],[2]. Since 1990, various standard practice management guidelines have been established, and surgical stabilization of rib fracture (SSRF) stands out as an evidence-based operative procedure [3]. This study highlights five cases of SSRF performed at Mackay Base Hospital (MBH), a regional hospital located in far North Queensland, almost 400 km from the nearest tertiary facility with a high incidence of chest trauma.
CASE SERIES
Case 1
A 78-year-old male, from home with wife, presented to the emergency department (ED) after an out-of-hospital cardiac arrest (OOHCA) and 45-minute cardiopulmonary resuscitation (CPR) by wife and paramedics. The patient returned to spontaneous circulation (ROSC) following CPR and intravenous (IV) adrenaline and was admitted to the intensive care unit (ICU) for further management. He also underwent coronary angiography with successful percutaneous coronary intervention (PCI) of the ostial left main coronary artery. Past medical history (PMHx) includes paroxysmal atrial fibrillation, on rivaroxaban and metoprolol.
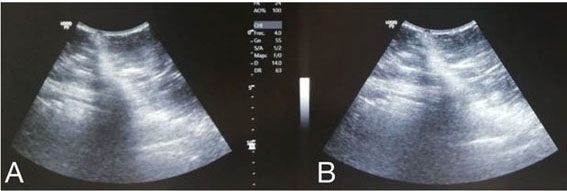
The initial computed tomography pulmonary angiogram (CTPA) showed bilateral CPR-induced anterior rib fractures (second to fifth), a large left-sided tension pneumothorax, and associated left-sided subcutaneous emphysema. Additionally, it demonstrated bilateral lower lobe consolidation, possibly aspiration pneumonia. Bilateral intercostal catheters (ICCs) were inserted as bedside ultrasonography also revealed a right-sided pneumothorax, and these were removed on day six after serial chest X-rays (CXRs) demonstrated resolution of pneumothoraces. However, CT chest on day 8 showed resolution of left-sided pneumothorax but demonstrated a fracture of the sternum with slight displacement, fractures at the costal cartilages of the right third to seventh ribs with mild to moderate pleural effusions, and pericardial effusions without signs of pneumomediastinum, which were previously unreported.
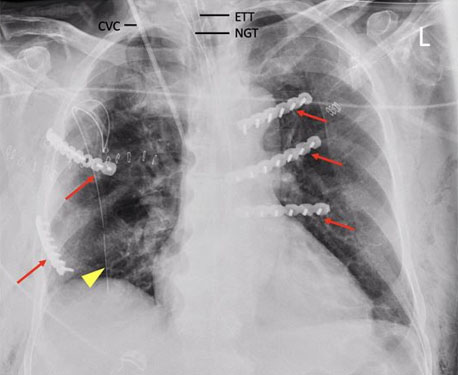
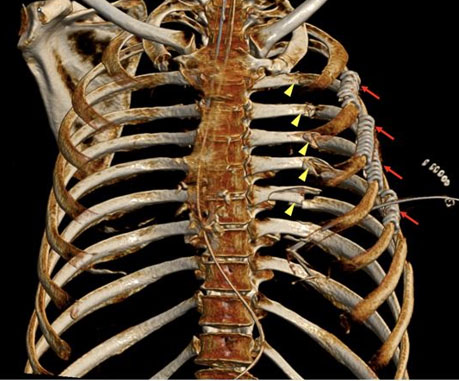
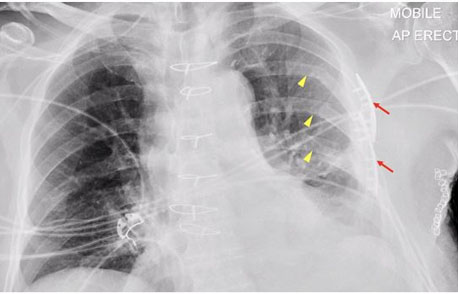
The patient was referred to General Surgery at this stage for consideration of SSRF due to difficulties weaning off ventilation. On post-trauma day 9, the patient underwent bilateral rib open reduction and internal fixation (ORIF) of right third, fifth, and left third to fifth ribs, for bilateral rib fractures with flail segments. The operation was performed under general anesthesia (GA) in the supine position in conjunction with the Orthopedic team. Bilateral parasternal incisions were made with a single lateral incision over the fifth rib. Synthes rib plates were applied, and 12-French (Fr) ICC replaced for right-sided pneumothorax encountered intraoperatively (Figure 1).
Extubation was successful two days postoperatively, and the chest drain was removed three days later. Unfortunately, the patient was palliated following an extensive family meeting, due to poor neurological recovery after extubation secondary to hypoxic brain injury, and passed away seven days postoperatively.
Case 2
A 59-year-old male presented with right-sided chest pain and difficulty breathing following a 2-m height fall from a ladder onto his right side chest. Past medical history includes type two diabetes mellitus (T2DM). He was also a heavy smoker and alcohol binge drinker.
The initial focused assessment with sonography in trauma (FAST) scan showed a right-sided pneumothorax. Computed tomography trauma pan-scan confirmed a right-sided pneumothorax with mild tension pneumothorax. There was radiological flail associated with posterior rib fractures (sixth to tenth) and lateral rib fractures (fourth to seventh). There were no other acute abnormalities in the brain, cervical spine, nor abdomen.
A 32-Fr ICC was inserted on the right chest in the ED, and patient-controlled analgesia (PCA) with oxycodone was commenced. The patient was admitted to the general surgical ward. Nil new injuries were identified from the tertiary survey.
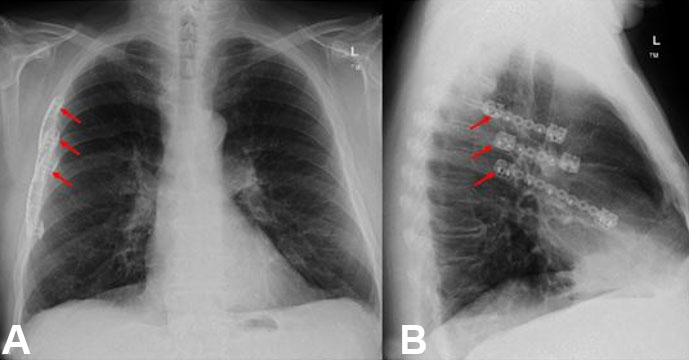
On the third day post-trauma, the patient underwent ORIF of the right anterior rib fractures (fifth, sixth) and anterior and posterior seventh rib fractures. The procedure was performed under GA in the left lateral position via left thoracotomy. Latissimus dorsi anterior muscle was retracted, and anterior serratus divided. Ribloc U+ plating system 150 mm was used for the seventh rib fracture, and 75 mm used for both fifth and sixth ribs (Figure 2 and Figure 3). Rib clamps aided reduction of fractures, and self-locking screws were placed. A new 20-Fr right-sided chest drain was placed.
The patient was admitted to ICU postoperatively. Thoracic epidural analgesia was placed in addition to oxycodone PCA being continued. The patient required a period of high-flow oxygen but was weaned to room air on postoperative day three. The ICC was removed on postoperative day two with no complications, and the patient was warded a day after. The patient was subsequently discharged home on day six with oral analgesia, with satisfactory recovery during his outpatient follow-up six weeks later.
Case 3
A 39-year-old male was brought in by ambulance (BIBA) after a fall from a horse with ICC to left chest inserted by paramedics on scene for a left-sided pneumothorax. Relevant PMHx included asthma and the recent commencement of amoxicillin for an infective exacerbation.
Focused assessment with sonography in trauma scan was negative, and initial CT showed multiple acute left-sided laterally displaced rib fractures (third to fourth), flail segments (fifth to seventh), posteriorly displaced fracture (eighth), and a small left hemopneumothorax associated with mild to moderate subcutaneous emphysema. There was no acute abdominopelvic pathology, spinal fractures, or intracranial hemorrhage (ICH).
Patient-controlled epidural analgesia (PCEA) was commenced in ICU. Intercostal catheters was removed post-trauma day three. However, the patient experienced ongoing suboptimal pain management despite an increasing rate of PCEA, adjunct morphine PCA, and a change to paravertebral block. Repeat CT chest demonstrated worsening displaced rib fractures and an interval increase of left-sided hemothorax. Therefore, the patient underwent ORIF on day 8. The anterolateral rib fractures were reduced with rib clips (Figure 4), and ICC inserted for ongoing hemothorax. The operative team decided fixation of posterior rib fractures was not required at the time.
The patient returned to the ICU intubated and had difficulty in ventilation secondary to a possible blocked ICC. The patient subsequently underwent a repeat CT chest, which showed possible pneumomediastinum and extensive subcutaneous emphysema. The ICC was replaced, and due to ICU concerns, the patient was transferred to a tertiary facility under a cardiothoracic unit. Bronchoscopy showed no evidence of tracheobronchial injury, and epidural analgesia was restarted with programmed intermittent epidural boluses (PIEB) in conjunction with PCA. The patient was then extubated on postoperative day 2 and warded on day 3. On postoperative day 5, the ICC was removed, PCA ceased, and the patient was discharged home with oral analgesia.
Case 4
A 56-year-old man was BIBA following a high-speed motorbike accident at 80 kilometers per hour (kph). The patient landed on his back onto sand, wearing safety gear and a helmet. Past medical history included right-sided inguinal hernia repair with mesh, carpal tunnel release, and depression.
Initial CT showed a right-sided radiological flail chest involving the third to seventh ribs and posterior rib fractures (eighth to twelfth). There was a small left apical pneumothorax and a small right-sided pleural effusion, likely hemothorax. Multiple fractures were reported, including a buckle-type fracture of the sternum, cervical and thoracic spinal fractures at multiple levels, right humeral head fracture, plus right acetabulum and inferior pubic rami fractures. No ICH nor abdominal injuries noted.
The patient was transferred to ICU, and oxycodone PCA commenced. On post-trauma day one, the patient developed hypoxia and required high-flow oxygen therapy due to worsening right-sided rib pain. The patient additionally received a regional block and ketamine infusion for pain control.
On post-trauma day 3, the patient underwent ORIF of the right-sided ribs (fourth to sixth). The patient had an episode of desaturation intraoperatively due to mucous plugging. The patient was repositioned from lateral to supine, and mucous plug suctioned via bronchoscopy. As a consequence, only anterior rib fixation proceeded. The Acumed Ribloc system was applied, and 50 mm plates were placed on each rib (fourth to sixth) with 2 screws on either side of the fracture for fixation (Figure 5). Intercostal catheters were inserted bilaterally.
Post-ORIF day 3, repeat CT chest showed a moderate left pneumothorax with a pleural catheter in situ and no right-sided pneumothorax. An additional left anterior ICC was inserted, and the right ICC removed. The left lateral ICC was removed post-ORIF day 4, and the left anterior ICC removed when serial CXRs demonstrated resolution. The patient also underwent ORIF of the proximal humerus, followed by cemented hemiarthroplasty of the shoulder. The patient was extubated and warded on post-rib ORIF day 8.
The patient elected to discharge against medical advice post-ORIF day 15 and was followed up in the outpatient clinic. The patient reported good recovery and participated well in outpatient physiotherapy.
Case 5
A 78-year-old male presented following blunt trauma versus cow with multiple blows to the left torso and a head strike against the fence. Left ICC was inserted in the local hospital due to desaturation and left-sided pneumothorax on X-ray. Past medical history includes coronary artery bypass graft (CABG), hypertension, gastro-esophageal reflux disease (GORD), and dyslipidemia.
Computed tomography trauma pan-scan showed left-sided rib fractures (fourth to eleventh) with a flail segment (fifth to seventh) and a small hemopneumothorax. There were also right-sided non-displaced rib fractures (third, fifth, eleventh). Additionally, CT showed small volume subdural hemorrhage, thickened terminal ileum with small volume hemorrhage, grade II splenic laceration without active bleeding, and superficial subcutaneous hematoma over the posterior lumbar, paraspinal, and gluteal regions.
The patient was admitted to ICU, and morphine PCA commenced. On post-trauma day 2, thoracic epidural analgesia was given for poor pain management despite PCA. On post-trauma day 3, the patient was intubated, and IV meropenem commenced due to febrile episode, increased oxygen requirement, and delirium. The patient subsequently underwent thoracotomy with left ORIF and ICC insertion. The Synthes Matrixrib set plate was placed on the left fourth and fifth ribs, and locking screws used for plate fixation (Figure 6). A left ICC was placed.
The patient was extubated post-ORIF day 2 and cleared on the tertiary survey. However, the patient developed another febrile episode and transaminitis post-operative day 3. The patient underwent transthoracic echocardiogram, CTPA, CT abdomen and pelvis, and CT brain, which revealed no new changes. On postoperative day 4, IV meropenem was ceased, and chest drain removed given clinical improvement. The patient was subsequently warded and discharged home on postoperative day 9 with oral analgesia and follow-up with his general practitioner (GP).

DISCUSSION
Overview of chest trauma
Chest trauma accounts for 25% of all traumarelated fatalities and contributes to an additional 25% of cases [4]. It has quickly risen to become the second most common traumatic injury in non-intentional trauma [5]. Chest trauma can result from penetrating or blunt trauma, with motor vehicle accidents being the primary cause, accounting for 70–80% of blunt trauma cases [6]. In Australasia and the UK, blunt injury is the cause of 90–95% of all chest trauma cases. Pulmonary contusions, pneumothorax, and hemothorax manifest in 30–50% of individuals experiencing severe blunt chest trauma [4]. Understanding the mechanism of injury in chest trauma is crucial, given that blunt and penetrating injuries exhibit distinct pathophysiology and clinical trajectories.
Scoring system
The STUdy of the Management of BLunt (STUMBL) chest wall trauma or Battle Score clinical prediction tool was initially created and externally validated to aid in the clinical decision-making process for patients involved with blunt chest trauma in the ED [7]. It incorporates risk factors such as age, number of rib fractures, chronic lung disease, pre-injury anticoagulant use, and oxygen saturation levels, which are utilized to estimate the likelihood of complications. The final risk scores range from 0-31+ and complications are broadly categorized as in-hospital mortality, morbidity (including all pulmonary complications), requirement for ICU admission, and prolonged hospital stay (seven or more days). In a review published in 2023, it was noted that the score’s clinical efficiency was evident, and its extensive utilization demonstrated the impact it exerts on clinical care, patient experience, and clinician decision-making [8].
Overview of SSRF
As outlined in the Chest Wall Injury Society Guideline for SSRF, over the past decade, the criteria for surgical stabilization of rib fixation (SSRF) have undergone changes, leading to increased utilization due to advancements in techniques and hardware [9]. One of the most extensively studied indications is chest wall instability, defined as either “flail chest,” characterized by the presence of at least three consecutive ribs fractured at two locations, or three consecutive ribs fractured with bicortical displacement.
Surgical stabilization of rib fracture is indicated in various scenarios reflecting chest wall instability, including three or more rib flail chest presentations (either radiographic or clinical), three or more offset ribs (displaced by 100% or more), instability or clicking motion upon palpation or as reported by the patient, three or more ipsilateral displaced fractures exceeding 50%, two or more pulmonary physiologic derangements such as a respiratory rate (RR) exceeding 20, an inspired spirometry measurement below 50% of predicted, a pain score surpassing 5 out of 10, or a poor cough [9]. Additionally, SSRF may be indicated in cases of failure to wean from mechanical ventilation beyond 48 hours or the development of specific indicators such as a rapid shallow breathing index (RSBI) exceeding 105, a respiratory rate surpassing 35, a heart rate exceeding 140, or oxygen saturation below 90%, coupled with signs of anxiety, diaphoresis, or agitation, all attributable to rib fractures [9]. The RSBI, which is calculated as RR divided by tidal volume, is the most widely used predictor of weaning success because it is easy to use and interpret [9].
However, there are absolute and relative contraindications to consider. Absolute contraindications include shock, hemodynamic instability, or ongoing resuscitation efforts, severe traumatic brain injury (TBI) or intracranial hypertension, acute myocardial infarction (AMI), and fractures occurring outside of ribs 3–10 [9]. Relative contraindications encompass patients aged 18 years or younger, those with significant comorbidities, mild to moderate TBI, respiratory compromise due to severe pulmonary laceration or contusion, unstable spinal or pelvic fractures, local infections such as empyema or mediastinitis, and a history of chest wall radiation [9]. These indications and contraindications are crucial in guiding the decision-making process for SSRF, as outlined in the Chest Wall Injury Society Guideline.
However, despite these indications, the implementation of SSRF remains low. Data from the National Trauma Data Bank show that only 1–2% of patients with flail chest undergo SSRF [10]. Several reasons contribute to this low rate, including a lack of familiarity with the operation among healthcare professionals, the absence of a uniform taxonomy that can be utilized to develop specific evidencebased guidelines, and the lack of specialty ownership of this disease process [10]. These factors highlight the need for greater awareness and understanding of SSRF among clinicians to ensure its appropriate use in eligible patients.
Surgical principles involve prioritizing higher severity injuries such as preoperative spinal injuries, open abdomen cases, significant vascular trauma, and pelvic external fixation [9]. The timing of SSRF is crucial, with immediate action required for flail chest cases, while procedures should ideally occur within 72 hours of injury to ensure easier reduction before callus formation [9]. However, SSRF may be delayed in cases of higher priority injuries [9]. Perioperative considerations include conducting CT reconstructions and preoperative or ontable ultrasound marking of fracture sites [9]. Optimal exposure is achieved through careful positioning and incision selection, such as lateral, inframammary, or posterior paramedian approaches [9]. Special approaches like video-assisted thoracoscopic surgery (VATS), bone grafting, or muscle xenografts may be advocated, along with anesthetic techniques like single-lung ventilation [9]. Muscle-sparing entry or division, particularly of the latissimus dorsi or trapezius muscles, is preferred [9]. The aim is to fix at least one end of the flail segment, either anteriorly or laterally, and staged procedures are recommended for unstable or bilateral cases [9]. Additionally, direct nerve blocks or paravertebral blocks may be employed, and new intercostal catheter insertions may be necessary to manage postoperative care effectively [9].
Evidence supporting SSRF demonstrates its significant benefits in reducing mortality and pulmonary complications. A meta-analysis by the Eastern Association for the Surgery of Trauma (EAST) of 22 studies involving 986 patients with flail chest, including 334 who underwent SSRF, revealed significant benefits [11]. Surgical stabilization of rib fracture in flail chest patients was linked to improved outcomes, including decreased mortality (odds ratio [OR] 0.3, 95% confidence interval [CI] 0.18−0.50, p<0.001), reduced duration of mechanical ventilation (weighted mean difference [WMD] −6.07, 95% CI, −9.27 to −2.89; p< 0.001), shorter ICU stay (WMD −4.21, 95% CI, −6.72 to −1.69; p=0.001), decreased hospital length of stay (LOS) (WMD, −7.63, 95% CI, −11.75 to −3.51; p<0.001), lower incidence of pneumonia (OR, 0.24, 95% CI, 0.13−0.46; p<0.001), and reduced need for tracheostomy (OR, 0.24, 95% CI, 0.12−0.50; p<0.001) [11]. However, analysis of nonflail patients was limited as no studies focused solely on nonflail rib fractures, and subgroup analysis in studies including both flail and nonflail rib fracture patterns was not conducted [11]. Additionally, a randomized prospective trial published in the Journal of the American College of Surgeons (JACS) found that patients undergoing operative fixation had significantly shorter ICU stays post-randomization (285 hours for the surgical group compared to 359 hours for the conservative group, p=0.03) and required less non-invasive ventilation after extubation (3 hours in the surgical group versus 50 hours in the conservative group, p=0.01) [12]. However, no differences in spirometry at 3 months or quality of life at 6 months were noted [12].
Although findings vary across studies, several authors have also reported a decrease in mortality rates. Tignanelli et al. conducted a retrospective analysis of more than 600,000 patients with rib fractures, assessing adherence to evidence-based practices from 2007 to 2014 across 777 US trauma centers in the National Trauma Data Bank [13]. Among 24,319 patients, 14% underwent SSRF, which was associated with a reduced mortality rate (odds ratio, OR, 0.13; 95% confidence interval, CI, 0.01–0.18; p<0.001) [13]. Furthermore, patients with rib fractures not meeting the flail chest criteria may also experience benefits from SSRF, such as decreased pain and improved quality of life, particularly for less displaced fractures [14]. Surgical stabilization of rib fracture has also been shown to be cost-effective. Predicted United States (US) Medicare costs were $17,162 for operative management compared to $22,537 for nonoperative management [15]. Tanaka et al. reported lower medical costs under Japanese public health insurance for patients who underwent operative fixation compared to those managed nonoperatively for severe flail chest ($13,455 vs. $23,423, p<0.05) [16]. These findings underscore the effectiveness of SSRF in improving patient outcomes and highlight its role as a valuable treatment option for traumatic rib fractures.
SSRF at MBH
Mackay Base Hospital, a large regional hospital, serves a population of over 125,000 and growing. The hospital faces a disproportionate burden of trauma, with incidents such as road traffic accidents, farming and mining accidents, and recreational injuries leading to a high incidence of rib fractures among patients. Complicating matters further is the fact that the closest cardiothoracic center is approximately 400 kilometers away in Townsville.
In 2021, a total of 172 patients presented to MBH ED with a coded diagnosis of rib fracture, with male dominance and a mean age of 56. Among these, 94 cases were classified as trauma activations, accounting for 55% of the total cases. Of the remaining cases, 78 were associated with lower risk mechanisms. Additionally, 61 admissions to the ED were subsequently discharged home. Notably, 78 patients were identified as having three or more rib fractures, representing 45.3% of the total rib fracture cases recorded. Additionally, 23 patients exhibited a radiological flail segment, comprising 13.4% of the total cases. In terms of SSRF procedures, there were five cases performed in 2021, resulting in an SSRF rate of 2.9%.
The challenges associated with patient retrieval include the cost and logistics involved, including the availability of services such as the Royal Flying Doctor Service and impact of weather conditions, which can cause delays in treatment. Additionally, there is a risk of patient deterioration during transit, and tertiary care bed availability, particularly in intensive care units, can be limited. Furthermore, some patients may prefer not to be transferred. Despite these challenges, MBH boasts a similar skill set and handles procedures of comparable complexity, further establishing its capability in managing such cases.
All five cases of SSRF involved male patients with a median age of 56 years (range 39–78 years). Among these cases, four were unilateral and one was bilateral. The mean surgical duration was 2 hours and 9 minutes, whilst mean anesthetic duration was 3 hours and 12 minutes. The number of ribs fixed ranged from 2 to 5. Following surgery, the median LOS in the ICU was three days (interquartile range [IQR] 2–6), with extubation occurring within 48 hours. The median hospital LOS postoperatively was six days (IQR 5.5–8). There was one reported morbidity and one mortality, both of which were not specific to surgery-related complications.
Recognizing the need for specialized surgical intervention, surgeons and orthopedic specialists at MBH actively engaged in upskilling through various avenues such as courses provided by the Australian and New Zealand Association for the Surgery of Trauma (ANZAST) and workshops conducted by surgical equipment suppliers. They underwent simulation training, cadaver procedures, and in vivo training to enhance their skills. Initially, equipment was sourced from Brisbane and delivered to MBH as needed, with orders fulfilled promptly for the next day. Presently, MBH has one set of equipment onsite, with plans underway to procure a second set to enhance capacity. Judicious patient selection is prioritized, and a multidisciplinary team approach involving surgeons, orthopedic specialists, anesthetists and their Anaesthesia Pain Service (APS) team, intensivists, nurses, and physiotherapists is adopted to ensure optimal patient care and outcomes.
However, several challenges have been identified in the process. Availability of equipment, including specialized instrumentation, remains crucial for conducting SSRF procedures effectively. However, there have been challenges in ensuring consistent availability of equipment at MBH. Additionally, there is limited surgical experience and technical expertise due to the relatively small number of cases performed to date. Patient positioning poses another significant consideration, especially in cases involving bilateral rib fractures, spinal, shoulder, pelvic fractures, and other associated injuries, which may complicate intraoperative management. Adequate intraoperative ventilation, coupled with precise positioning, is essential for successful surgery. Accessing difficult fracture sites, such as those located under the scapula, presents further challenges during the procedure. Furthermore, there is variable interest among surgeons regarding performing SSRF, reflecting the diverse perspectives and experiences within the surgical team.
Moving forward, our goals include the development of locally tailored guidelines to optimize our SSRF procedures. We aim to expand our case numbers and broaden the indications for surgery to encompass a wider range of patients who could benefit from this intervention. Additionally, we are committed to upskilling surgeons who show interest in performing SSRF procedures through targeted training and educational programs. Refinement of our surgical techniques and hardware will be an ongoing focus to ensure optimal patient outcomes. Seeking advice and fostering communication with high-volume centers will be essential for staying updated on best practices. Regular audits of our outcomes will be conducted to monitor our performance and identify areas for improvement. Collaboration and teamwork among all members of the healthcare team will remain fundamental to our approach. Research studies comparing different surgical techniques, such as Judet struts versus metal or resorbable plates, would further enhance our understanding and refine our practices.
LIMITATIONS
This case series is limited by its small sample size, comprising only five SSRF cases over an 18-month period, which restricts the statistical power and generalizability of the findings. Additionally, the absence of a conservatively managed comparator group limits our ability to directly assess the relative efficacy of SSRF. Future studies incorporating propensity score matching or establishing regional SSRF registries may provide more robust comparisons and enhance generalizability. As a single-center study conducted in a regional hospital, outcomes and operative times may also be influenced by the learning curve and variability in equipment availability, potentially differing from those in high-volume tertiary centers. Future directions to address these limitations include the development of a regional SSRF registry, longitudinal patient follow-up incorporating pain scores and return-to-work data, and multicenter collaborations for pooled data analysis. Incorporating methods such as propensity score matching in future retrospective studies may also enable more rigorous comparison between operative and conservative management strategies.
CONCLUSION
The strategic combination of surgical expertise and logistical considerations, including the limitations in transporting patients to the nearest cardiothoracic resuscitation center, positions MBH as a fitting institution for SSRF. This case series highlights favorable postoperative outcomes, such as early extubation, manageable ICU stay, and low complication rates, demonstrating the clinical feasibility of SSRF in regional centers. Moving forward, development of tailored regional guidelines, investment in surgeon training, and stronger collaboration with tertiary centers will be essential to broaden access and build a sustainable SSRF service. Larger, multicenter studies are recommended to further evaluate long-term outcomes and validate these findings.
REFERENCES
1.
Gaillard M, Hervé C, Mandin L, Raynaud P. Mortality prognostic factors in chest injury. J Trauma 1990;30(1):93–6. [CrossRef]
[Pubmed]

2.
Sharma OP, Oswanski MF, Jolly S, Lauer SK, Dressel R, Stombaugh HA. Perils of rib fractures. Am Surg 2008;74(4):310–4. [CrossRef]
[Pubmed]
3.
Brasel KJ, Moore EE, Albrecht RA, deMoya M, Schreiber M, Karmy-Jones R, et al. Western Trauma Association Critical Decisions in Trauma: Management of rib fractures. J Trauma Acute Care Surg 2017;82(1):200–3. [CrossRef]
[Pubmed]
4.
Fitzgerald M, Gocentas R, Stevens J. Chest trauma. In: Cameron P, Jelinek G, Kelly AM, Brown A, Little M, editors. Textbook of adult emergency medicine. 4th ed. Elsevier; 2015.
5.
Jain A, Waseem M. Chest trauma. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025.
[Pubmed]
6.
Morley EJ, Johnson S, Leibner E, Shahid J. Emergency department evaluation and management of blunt chest and lung trauma (Trauma CME). Emerg Med Pract 2016;18(6):1–20.
[Pubmed]
7.
Battle C, Hutchings H, Lovett S, Bouamra O, Jones S, Sen A, et al. Predicting outcomes after blunt chest wall trauma: Development and external validation of a new prognostic model. Crit Care 2014;18(3):R98. [CrossRef]
[Pubmed]
8.
Battle C, Cole E, Whelan R, Baker E. Scoping review of the literature to ascertain how the STUMBL Score clinical prediction model is used to manage patients with blunt chest wall trauma in emergency care. Injury 2023;54(7):110796. [CrossRef]
[Pubmed]
9.
Delaplain PT, Schubl SD, Pieracci FM, Shen A, Brabender DE, Loftus J, et al. Chest Wall Injury Society Guideline for SSRF: Indications, contraindications and timing. Chest Wall Injury Society; 2020.
10.
Fokin AA, Wycech J, Weisz R, Puente I. Outcome analysis of surgical stabilization of rib fractures in trauma patients. J Orthop Trauma 2019;33(1):3–8. [CrossRef]
[Pubmed]
11.
Kasotakis G, Hasenboehler EA, Streib EW, Patel N, Patel MB, Alarcon L, et al. Operative fixation of rib fractures after blunt trauma: A practice management guideline from the Eastern Association for the Surgery of Trauma. J Trauma Acute Care Surg 2017;82(3):618–26. [CrossRef]
[Pubmed]
12.
Marasco SF, Davies AR, Cooper J, Varma D, Bennett V, Nevill R, et al. Prospective randomized controlled trial of operative rib fixation in traumatic flail chest. J Am Coll Surg 2013;216(5):924–32 [CrossRef]
[Pubmed]
13.
Tignanelli CJ, Rix A, Napolitano LM, Hemmila MR, Ma S, Kummerfeld E. Association between adherence to evidence-based practices for treatment of patients with traumatic rib fractures and mortality rates among US trauma centers. JAMA Netw Open 2020;3(3):e201316. [CrossRef]
[Pubmed]
14.
Sedaghat N, Chiong C, Tjahjono R, Hsu J. Early outcomes of surgical stabilisation of traumatic rib fractures: Single-center review with a real-world evidence perspective. J Surg Res 2021;264:222–9. [CrossRef]
[Pubmed]
15.
Swart E, Laratta J, Slobogean G, Mehta S. Operative treatment of rib fractures in flail chest injuries: A meta-analysis and cost-effective [CrossRef]
[Pubmed]
16.
Tanaka H, Yukioka T, Yamaguti Y, Shimizu S, Goto H, Matsuda H, et al. Surgical stabilization of internal pneumatic stabilization? A prospective randomized study of management of severe flail chest patients. J Trauma 2002;52(4):727–32. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Imeshi Indigahawela - Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Weiwei Shi - Analysis of data, Interpretation of data, Drafting the article, Final approval of the version to be published
Xin Yi Goai - Substantial contributions to conception and design, Acquisition of data, Revising it critically for important intellectual content, Final approval of the version to be published
Constantin Dlaska - Substantial contributions to conception and design, Revising it critically for important intellectual content, Final approval of the version to be published
Mahanama Dissanayake - Analysis of data, Interpretation of data, Drafting the article, Final approval of the version to be published
Casper Pretorius - Substantial contributions to conception and design, Interpretation of data, Revising it critically for important intellectual content, Final approval of the version to be published
Christian Beardsley - Substantial contributions to conception and design, Revising it critically for important intellectual content, Final approval of the version to be published
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Imeshi Indigahawela et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.